ACL Surgery Recovery
ACL Injury
Have you torn the ACL (anterior cruciate ligament) in your knee, and are wondering what recovering from ACL surgery might be like?
Maybe you’ve injured your knee and it keeps giving way, and you’re worried you might have torn your ACL?
Perhaps you’re facing ACL reconstruction surgery and want to make the very best recovery?
Or, are you someone who’s struggling to get back to sport after ACL surgery, despite doing lots of physio?
If so, you’re in the right place.
Let’s talk about:
- What it’s like to tear your ACL
- Whether ACL reconstruction may (or may not) be right for you
- What to expect after ACL reconstruction surgery
- How to know if you’re ready for sport
- Why you might not be recovering – 7 common ACL rehab mistakes
But first, let’s consider the success of ACL reconstruction surgery (especially since, if it’s going to be a long rehab journey, you want to know it’s worth it, right?).
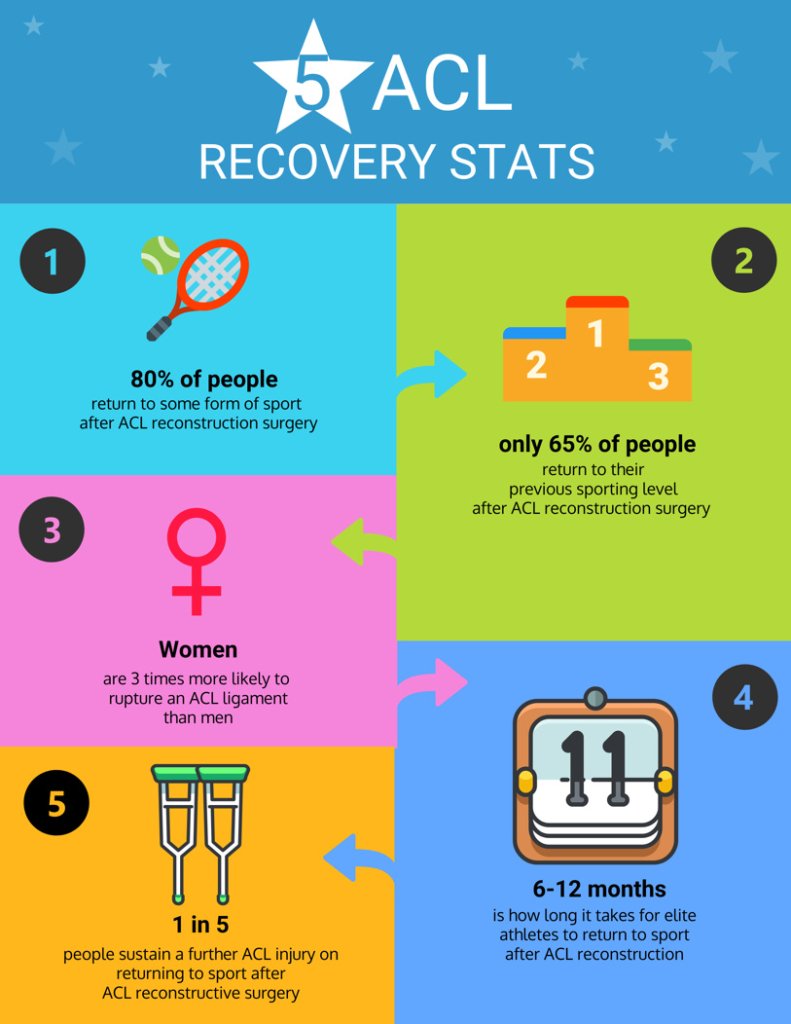
If you’re an elite athlete, a meta-analysis of many studies has shown that the likelihood of you successfully returning to the same level of sport after an ACL reconstruction, is around 82%.
Even for elite athletes, recovery takes a long time (6-12 months) – despite having the best medical teams around them, and often being paid to do the rehab.
But what if you’re not an elite athlete?
Well, you still have an 80% chance of returning to some form of sport, but only around a 65% chance of getting back to the same level of sport you were at pre-injury.
There is also a risk of re-tearing your (reconstructed) ACL, which is somewhere between 20- 25%. If you’re female, your risk of a further ACL injury after reconstruction surgery is FIVE times higher, than if you’d never had an ACL tear.
There’s clearly a big gap between the success rates of pro-athletes, compared with the success rates for us mere mortals. This is partly because life gets in the way, and ACL rehab is hard, time-consuming work, but the quality of the physiotherapy and rehab can play a significant part..
A review of the data also shows that it is not just due to physical limitations but that there are strong psychological factors that also contribute to people not getting back to their pre injury performance.
The good news here is that following an ACL focused rehab programme with a specialist physio = an excellent outcome (even if you’re not an athlete).
What’s it like to tear your ACL?
I’m an actress and stunt performer, and the day I tore my ACL, my trainer asked me to perform a risky manoeuvre of repeatedly jumping on one leg with the other leg held up in the air.
The dynamics of the movement felt wrong, and when I landed, my knee collapsed. I managed to get up off the ground, and I felt pressure to continue the session; after performing a kick, I knew my knee was in serious trouble.
Mike stayed late at the clinic to see me, and after his assessment, he arranged an urgent MRI scan for me (and even phoned me on a Sunday to share the results).
I was naturally worried because my livelihood was at stake, but even though the news was bad, Mike reassured me that we’d get through it, and he’d get me back into action; and he was true to his word.
Fran Katz, Actress and Stunt Performer
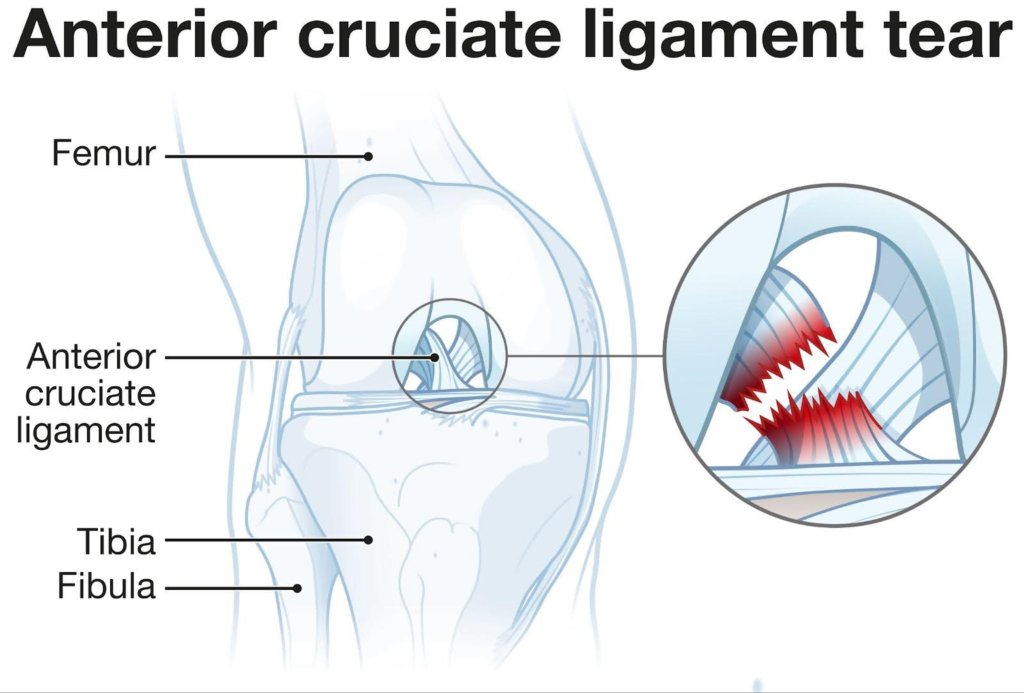
The ACL (anterior cruciate ligament) is a ligament that’s located deep within your knee that provides a very important stability component. It essentially works to keep your knee in alignment, by preventing the shin bone from moving too far forwards on the thigh bone, and it also helps to reduce excessive rotation, hyperextension, and side-to-side movements of the knee joint.
Most ACL injuries tend to happen during a sport or activity that involves a sudden change of direction at the knee (e.g. falling badly when skiing), or jumping and landing awkwardly (e.g. during football or netball).
If you’ve torn your ACL, you might experience:
- hearing or feeling a ‘pop’ within your knee
- sudden onset of pain (although not always)
- difficulty getting up if you’ve fallen
- difficulty bearing weight on your leg
- rapid swelling of your knee
- knee giving way, or feeling unstable
When Your Knee “Just Doesn’t Feel Right”
Many people who sustain an ACL injury describe a very clear moment when they knew something wasn’t right. The knee may have twisted, shifted or given way, followed by swelling and a sense of instability. From that point on, it can feel untrustworthy; particularly when walking downstairs, pivoting or changing direction.
If this sounds familiar, you may have attended A&E. Often an X-ray is performed to rule out a fracture, and you’re advised to rest, ice and elevate the knee, with instructions to see your GP if symptoms persist.
At this stage, many people feel uncertain about what to do next.
A Structured Clinical Assessment
At Complete Physio, we begin with a detailed and methodical assessment.
We take the time to understand:
- The exact mechanism of injury
- How your knee has behaved since the incident
- Any previous knee injuries or medical history
- How the problem is affecting your work, sport and daily life
A thorough physical examination follows:
We assess swelling, joint line tenderness and signs of instability using recognised clinical tests such as the Lachman and anterior drawer tests.
We also test muscle activation, particularly quadriceps control, and movement quality through functional tasks such as single-leg squats, step-downs and, where appropriate, hopping or jumping.
This combination of history, examination and functional testing helps us determine the likelihood of an ACL injury and identify any associated deficits.
At Complete Physio, we also offer a High Performance Testing service for individuals who want to get back to a higher level of activity. This testing package combines Force Plate Testing and Fixed Dynamometry to provide a comprehensive assessment of your physical capabilities.
The Role of Imaging
If clinical findings suggest a possible ACL tear, we will recommend an MRI scan.
While X-rays are useful to exclude fractures, and ultrasound can assess superficial soft tissues, neither is sufficient to evaluate deeper intra-articular structures.
MRI remains the gold standard for confirming an ACL injury and identifying associated damage.
ACL tears commonly occur alongside other injuries, including:
- Meniscal tears (the fibrocartilage ‘shock absorbers’ between the femur and tibia)
- Medial collateral ligament (MCL) injury
- Articular cartilage damage
- Bone bruising
Understanding the full extent of injury is essential in guiding the most appropriate management plan.
At Complete Physio we can arrange for you to have an MRI scan with one of our recommended imaging centres, without the need of a GP referral.
Treatment Options: Surgery vs Rehabilitation
If an ACL rupture is confirmed, there are broadly two management pathways:
1. Surgical Reconstruction
This involves reconstructing the ACL using a tendon graft (commonly from the hamstring or patellar tendon), followed by a structured and progressive rehabilitation programme.
2. Non-Surgical Rehabilitation
Some individuals can achieve excellent outcomes through high-quality, progressive physiotherapy alone. This approach focuses on restoring strength, neuromuscular control, confidence and sport-specific function.
ACL reconstruction is an excellent option for some patients, particularly those returning to pivoting sports, but it is not always necessary or appropriate for everyone.
Decisions should be based on your own goals, lifestyle demands, knee stability and personal preferences.
Specialist Guidance at Every Stage
You may choose to seek input from a knee surgeon or sports medicine consultant to explore your options fully. At Complete Physio, we work closely with leading orthopaedic and sports medicine specialists to ensure you receive clear, evidence-based advice.
Our role is to guide you through the uncertainty, provide expert assessment, and help you make informed decisions about the best path forward; whether that involves surgery, rehabilitation, or a carefully planned combination of both.
Should I have ACL surgery?
Many factors influence the decision around whether (or not) to have surgery for your ACL tear, and you’ll want to spend some time thinking about this and getting advice.
There’s no rush to have to make a sudden decision about this. It’s always best to get your knee into optimal condition (prehabilitation) before having surgery, so you’re not going to ‘miss the boat’.
You might want to consider ACL construction surgery if:
- Your knee is fundamentally unstable and it’s making everyday life awkward
- You’ve also damaged other structures within the knee (such as the menisci or joint surfaces)
- You want to return to sports that require jumping, pivoting, and turning, (such as netball, football, rugby, skiing, martial arts, and gymnastics)
- You’re prepared to put in the time and effort to do the rehab
ACL reconstruction surgery may not be in your best interests (or necessary) if:
- You’ve only partially torn your ACL, and your knee isn’t unstable
- You’ve significant osteoarthritis (wear and tear) within your knee
- You’re not interested in pivoting or twisting sports
- You’re not well enough medically to undergo surgery
- You recognise that you’re not going to be able to fully engage in the rehab that’s required.
A good number of people, who have undergone extensive Physio led rehab, can happily return to ‘straight line’ activities, such as running and cycling, without undergoing ACL reconstruction. And in some cases people manage to return to a level of sports such as netball, football, skiing etc that they are happy with.
When I tore my ACL, I didn’t experience any pain, but my knee didn’t ‘feel right’. I spent several weeks doing rehab and exploring what was possible in terms of activity. In the end, when I did decide to go ahead with surgery, my knee was really well prepared for it.
If you’re undecided about whether to have surgery, you’ve nothing to lose, and everything to gain, by going through rehab first (even if it eventually turns out to be prehab!)
Prehabilitation before ACL reconstruction surgery
To undergo ACL reconstruction surgery, your knee needs to be in the best shape possible:
- Your knee should be comfortable and not swollen
- Your knee should ideally have a full range of movement
- Your quads muscles should be strong and firing well
It’s so important to have well-functioning quads going into ACL surgery.
When you injure your knee and it swells, the quads shut down and decline in terms of their strength and firing rates.
Studies have shown that if you have a preoperative quads strength deficit going into surgery, it will have a negative outcome on the function you can achieve one year after the operation (even if you try to make up the deficit after the surgery).
In other words, it’s a no-brainer to get your quads as best prepared as possible before surgery.
What to expect after ACL reconstruction surgery
Rehab after ACL reconstruction
Most ACL reconstruction occurs as a day case surgery, meaning you get to go home on the same day. It’s not possible to stitch the ends of the ACL back together once it’s torn, and so the ACL is ‘reconstructed’ using a tendon which is typically harvested from either your own hamstring muscle (although patella tendon grafts are sometimes used), or from a donor tendon.
Holes are drilled into the tibia (shin bone) and femur (thigh bone) and the graft is threaded through and fixed in place with screws. It’s all done through keyhole incisions, which are less than a centimetre in size.
Most surgeons will encourage you to start loading weight onto your leg on day one and to start walking if comfort allows. You’ll likely use crutches for a few days, to give your knee a little support.
This is when the hard work begins!
The initial rehab goals are to get the swelling down, get the knee fully extending, and get good activation of the quads and hamstring muscles.
How much time will I need to devote to doing my rehab exercises?
It takes commitment to do your rehab exercises, but it is possible to fit this in alongside a busy work and family life if you plan well..
In the first month, it’s all about little and often; low-intensity amounts of exercise, e.g. 10-15 minutes, carried out 3 or 4 times a day. You could do your first little session before you start work at your desk, then another at coffee break time, lunchtime, and at the end of the day.
As your rehab progresses the physicality of the exercises becomes more intense, and that means, you’ll need more recovery time in between. In terms of commitment, this could look like 40 minutes, 3 times per week.
ACL recovery mistake #1- Not being prepared for surgery
It’s my experience that many patients don’t get optimal prehab before surgery, and some go into surgery too soon.
There is a tendency for surgery to be offered six weeks after the date of the injury, but what if you’re not yet sufficiently prepared?
Take your time and do the necessary prehab, first.
ACL Rehab Mistake #2: Avoiding Open-Chain Quad Strengthening
There has been much controversy over the years about the right kind of exercise to get your quads into good shape. A lot of debate exists about ‘open chain’ and ‘closed chain’ quads exercises.
Closed chain exercises are ones where your foot is either in contact with the ground (e.g. during a squat) or fixed to an object (such as a spin bike pedal). Open chain quads exercises are ones where your foot is not on the ground and is free in the air (e.g. knee extension exercises).
Some surgeons have prescriptive protocols for how they want a patient’s rehab to be progressed, and there has been a vogue in the past for open chain exercises to be banned.
The thinking behind this was that too much load might be placed across the new ACL graft, potentially leading to it being overly stretched.
On the flip side, open chain exercises such as seated leg extensions, are an excellent way to build quads strength.
Thankfully, the up-to-date advice is shifting; open chain quads exercises initiated from six weeks post-surgery improve strength and don’t adversely affect the ACL graft.
ACL recovery mistake #3 - Not testing progress frequently enough
How do you know if you’re really progressing during rehab?
The answer is that we have to test, test, and test again. Too often I see patients who are following a generic, ‘one-size fits all’ protocol, which is typically time-based and doesn’t take into account how well the patient is actually progressing, and what their individual goals are.
What do I mean by testing?
It’s looking at pain levels, joint swelling, tolerance and sensitivity to activities, how well thigh muscles are being recruited, the execution of squatting and jumping, and how well landing is controlled, each and every time the person comes to the clinic.
At compete we have a High Performance Testing Service which combines Force Plate Testing and Fixed Dynamometry to provide a comprehensive assessment of your physical capabilities.
This is particularly important in the later stages of rehab, when planning a return to sport.
I’ll be looking to see how well the person performs the following:
- Single leg vertical hop test
- Single leg drop test
- Triple hop test
- Y Balance test
These tests will tell me whether a person is physically prepared to start planning a return to sport, and they are important because the research shows that performing poorly in these tests equates to a significant increase in the risk of an ACL re-tear.
ACL recovery mistake #4 - Neglecting your hamstrings
If you’ve had an ACL reconstruction with a hamstring graft, your body will try to make good on the tendon loss, through a tendon regeneration process. Studies estimate that this process occurs in around ¾ of patients within the first year after the hamstring tendon was harvested.
Not unsurprisingly, many people experience power deficits and altered biomechanics as a result of the tendon graft being harvested from their hammy. It’s also common to experience hammy pain.
Your physio must focus time on hamstring rehab. Sometimes there’s a tendency for the focus to be all about quads strengthening, and the hammy strengthening gets overshadowed. This is a problem because we know that loss of strength in knee flexion (the role of the hamstrings) increases the risk of ACL re-injury.
ACL recovery mistake #5 - Return to sport rehab is too generic
No two bodies are the same and no two sports are the same.
The rehab you’ll need if you love Brazilian Jiu-Jitsu is very different to the rehab you’ll need if you’re a five-a-side footballer.
Sometimes a person’s rehab stops after the ‘you’re ready to start jogging’ phase, or if their health insurance deems that returning to sport is a ‘bit of a luxury’.
A successful return to the activities you love means that you can meet all the functional requirements of the sport you’ll be playing, and that requires that your physio has an excellent working knowledge of the demands of your sport and factors them into your rehab.
ACL recovery mistake #6 - Not including sufficient perturbation training
When we participate in sport, we may be moving around on uneven terrain, and potentially colliding with other individuals.
To prevent injury and to perform well, we need a high level of reactive balance. It’s our ability to be able to right ourselves, or control our centre of gravity, when we’re about to lose our balance or if we are landing from a jump in an unexpected manner.
In other words, it’s about controlling movement we weren’t anticipating.
Studies have shown that people who’ve had ACL surgery are overly reliant on their vision to correct the imbalance, and they particularly need to regain good activation of the proprioceptive system (this is the kinaesthetic system that enables the body to ‘feel’ where it is in space).
The good news is that perturbation training (aka reactive balance training) can help us to rapidly re-learn this skill, particularly if we reduce the amount of visual information the brain is receiving (e.g. with eyes closed exercises).
ACL recovery mistake #7 - Not getting your head in the right place
It’s very natural to feel a little concerned about how your knee will handle returning to sport. Many people have fears about the risk of re-injuring their knee, and it’s a significant factor in why some people never make it back to sport.
Psychological readiness is key when returning to sport successfully, so as well as preparing the body, we need to prepare the mind, and a big part of this is goal setting.
During ACL rehab, we set weekly goals (e.g. in the first week post-op, the goal might be to achieve full extension) and we document achieving these goals. Because it’s a long rehab journey, it’s important to be able to look back and see how much you’ve achieved, and it’s my job to help maintain motivation in this process.
Knowing you’ve done all the hard work, and have gone through all the necessary rehab stages, as well as proving yourself to be physically capable, is very empowering, and it will enable you to truly feel ready to return to sport.
“I’ve previously torn my other ACL, and the experience of rehab with Mike was beyond amazing. I’m an athlete and Mike gave me the confidence to trust my body and progress swiftly.
His experience of working with athletes and elite performers means he has an excellent understanding of the demands placed on my body. Not only do I need to be strong, but my dance movements need to be aesthetically pleasing too. Mike made absolutely sure that I could fully and gracefully take my knee to full extension.
Throughout my rehab, Mike gave me confidence, he pushed me when I needed it, and he was immensely patient with me through the ups and downs. He was in constant communication with my surgeon, and I felt so supported. I’m getting ready to return to work, and if you’re going through an ACL recovery, I cannot recommend Mike enough!”
Fran Katz, Actress and Stunt Performer
This article was written by Mike Brent. Mike is a highly specialised physiotherapist, who works at our Angel and Swiss Cottage clinics.
Mike has worked in professional rugby to return players to elite sport, and has twice been an ACL injury patient himself, experiencing all the emotional ups and downs it brings.
If you have torn your ACL, are considering ACL surgery, or if you’re not getting the results you need from your rehab, book an appointment to work with Mike, to get you back to the sport you love!
Ready to take the next step in your rehabilitation? Email info@complete-physio.co.uk or call 020 7492 3875 to book your session today!
References
- Ardern CL, Webster KE, Taylor NF, et al. Return to sport following anterior cruciate ligament reconstruction surgery: a systematic review and meta-analysis of the state of play
British Journal of Sports Medicine 2011;45:596-606. - Grindem H, Snyder-Mackler L, Moksnes H, et al. Simple decision rules can reduce reinjury risk by 84 % after ACL reconstruction: the Delaware-Oslo ACL cohort study. Br J Sports Med. 2016;50(13):804–8.
- Paterno, M.V., Rauh, M.J., Schmitt, L.C., Ford, K.R. and Hewett, T.E., 2014. Incidence of Second ACL Injuries 2 Years After Primary ACL Reconstruction and Return to Sport. Am J Sports Med, 42(7), pp.1567-1573.
Wright, R.W., Haas, A.K., Anderson, J., Calabrese, G., Cavanaugh, J., Hewett, T.E., Lorring, D., McKenzie, C., Preston, E., Williams, G. and MOON Group, 2015. Anterior Cruciate Ligament Reconstruction Rehabilitation: MOON Guidelines. Sports Health, 7(3), p.239.