Meniscus Injuries – Everything you need to Know

What is a meniscal tear?
A meniscal tear is an injury to a part of your knee called the meniscus. Two pieces of cartilage sit inside your knee, between your thigh bone (femur) and shinbone (tibia). This cartilage is the meniscus.
The meniscal cartilages are at risk of tearing due to their constant exposure to repetitive loading as we walk, run or perform other activities.
A torn meniscus is one of the most common knee injuries. Any activity that causes you to forcefully twist or rotate your knee, especially when putting your full weight on it, can lead to a torn meniscus.
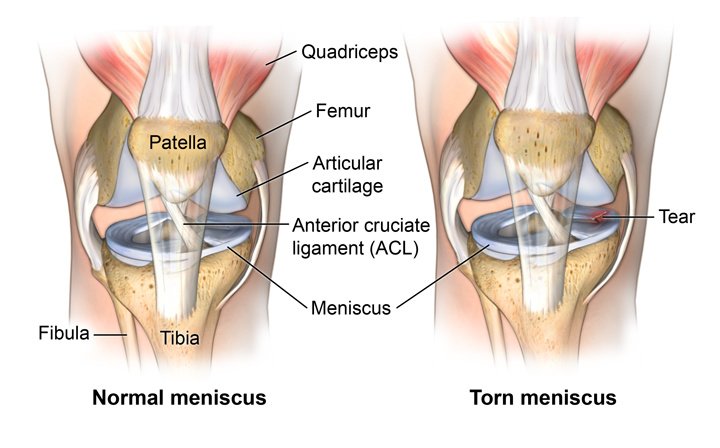
Knee Joint and Meniscus Anatomy
The knee is made up of the femur (thigh bone), the tibia (lower leg bone), and the patella (knee cap). Ligaments and tendons connect the femur to the bones of the lower leg. The four main ligaments in the knee attach to the bones and act like strong ropes to hold the bones together.
Every joint in the body is lined by extremely smooth tissue called “articular cartilage.” The articular cartilage of the knee coats the end of the femur (thigh bone), the top surface of the tibia (shin bone) and the back surface of the patella (kneecap).
In addition to articular cartilage, the knee joint also has meniscal cartilages, which are specialised pieces of tissue that act as shock absorbers.
You have two menisci in each knee called the ‘medial’ and ‘lateral’ meniscus. The menisci are thick, wedged, C-shaped, rubber like pads of cartilage tissue. As we walk, run, and jump, the knee absorbs tremendous forces. It is the shock absorbing capacity of the meniscus that protects the articular cartilage from wear and tear, and reduces the risk of developing knee osteoarthritis.
In addition to their role as a ‘shock absorber’, the wedge shape assists with the knee’s rotational stability and they also help to lubricate the joint and improve smooth movement of the knee.
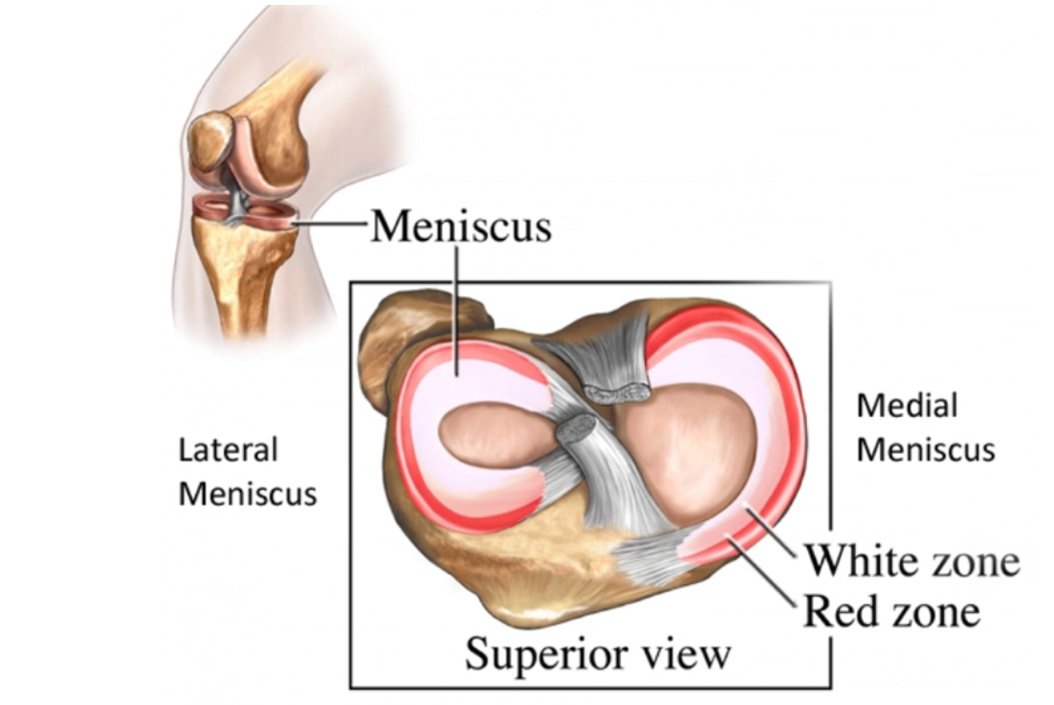
As you can see from the diagram above, there is an outer and inner portion of the meniscus. The outer parts of the meniscus have adequate blood supply, but the middle and inner parts have poor blood supply. Because blood supply can affect healing, the location of a tear will affect treatment options and management.
The main important functions of the meniscus are:
- Shock absorption
- Load transmission (spreading weight more evenly throughout the knee joint)
- Increasing knee joint stability
- Joint lubrication
What causes a meniscal tear?
There are two ways in which your meniscus can be injured, either through trauma or degeneration.
Traumatic meniscal tears typically happen to those aged under 40 years old and are associated with a twisting or turning movement whilst your foot is planted on the floor. In a young sporty person this could be due to turning quickly when playing a game of football, or a tackle during a rugby match. It is also a common skiing injury. The effect of this twisting movement puts torsion throughout the meniscus and causes the fibres to tear. Some people report they hear their knee click and often feel pain immediately.
Degenerative meniscus lesions are common in those who are middle-aged or older, they do not need a specific injury or incident. They can gradually occur and worsen slowly over several months or years. The risk increases with age, obesity, lack of strength or reduced flexibility.
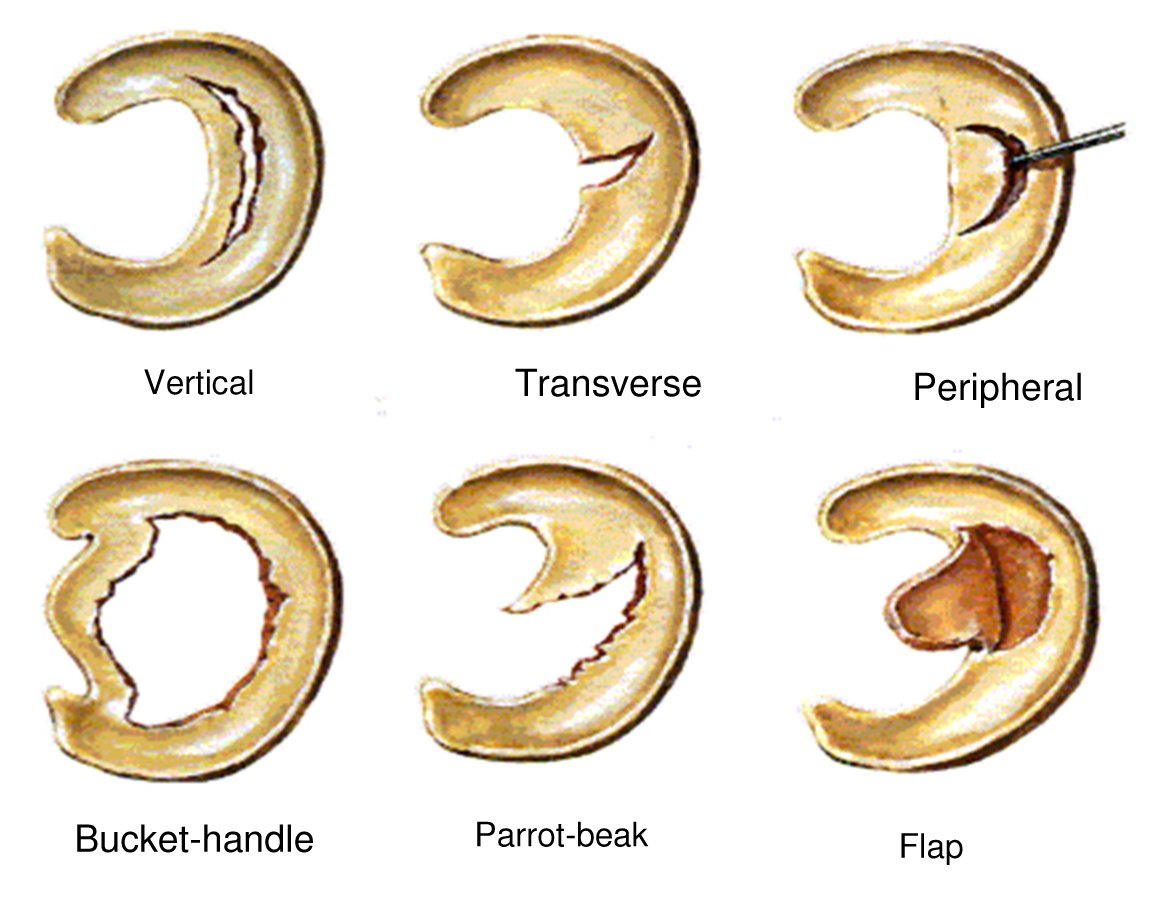
There are many different types of tears (see image below). The different tears can present with their own specific symptoms. Meniscal tears can also occur in combination with tears of ligaments around the knee e.g., an ACL tear (add link when ACL page is live)
Types of meniscal tears
What are the symptoms of a meniscus tear?
Torn meniscus symptoms typically start with a mechanism of injury that involves a history of a painful twist occurring on a slightly bent knee. Degenerative meniscus tears can present slowly with less obvious signs.
The pain from a meniscal tear is often localised to the inner or outer part of the knee joint, and less so at the front of the joint.
Patients often describe pain with bending and twisting, and sometimes pain at night. Often people with meniscal tears complain of stiffness and recurrent swelling of the knee joint.
Some meniscal tears are large and a fragment of the damaged meniscus may loosen partially and drift into the knee joint between the tibia and femur bone. When this occurs the fragment may cause a block to movement and the knee becomes ‘locked’, limiting your ability to fully straighten or fully bend your knee.
The symptoms can vary from person to person but the key signs and symptoms are:
- Swelling and stiffness – this normally takes 24 hours to develop after the onset of injury, however can be more gradual in the case of degenerative tears.
- Tenderness on the inside (medial meniscus tear) or outside (lateral meniscus tear) of the knee
- Pain with fully straightening or fully bending the knee
- Locking or catching of the knee
- Pain at night
- Pain whilst squatting, twisting and kneeling
- Feeling of instability or the knee giving way
If you are experiencing any of these symptoms, or suspect that you have a meniscus injury, and would like to see one of our expert physiotherapists you can call 0207 482 3875 or email info@complete-physio.co.uk. If you would like to speak to a specialist before booking, then please send us an email with your details and we will call you back.
How is a meniscal tear diagnosed?
Meniscal tears are quite straightforward to diagnose. Clinical assessment has been shown to be around 80% accurate for diagnosis of meniscus tears.
At Complete Physio our highly experienced physiotherapists will carry out a comprehensive assessment of your knee joint.
Your physiotherapist will firstly ask questions about your injury, past health, symptoms, and exercise regime.
After your consultation, your physio will complete a series of clinical tests to help develop a diagnosis; these may include:
- Measuring the range of movement of your knee.
- Assessing muscle strength, specifically the quadriceps in your knee and also the muscles around your lower leg and hips.
- Assessing muscle length and flexibility of quadriceps, hamstrings and calfs.
- Watching you move your knee and how you perform activities such as squatting, hopping, jumping, running.
- Gently, but skilfully, feeling around your knee joint to find exactly where it is most painful.
- Functional tests - if your pain is present during a specific activity or task, you may be asked to perform these, so the physiotherapist can assess exactly what is aggravating your pain.
- There is a specific meniscal test called the ‘McMurray’s test’ that your physiotherapist may additionally carry out to help establish your diagnosis.
Research has shown an increased risk of early onset of arthritis after damaging your meniscus and therefore an accurate diagnosis and appropriate treatment is paramount to a positive outcome.
Will I need a scan?
MRI
If we are unsure of your diagnosis or we would like to understand more about the extent and type of the meniscal tear, then we may refer you for an MRI scan. MRI scans are also very useful to assess for any other contributing factors such as an associated ligament tear. We can refer you directly without going to your GP.

Diagnostic Ultrasound
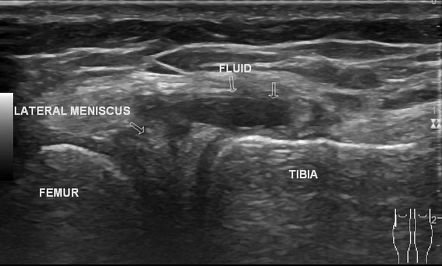
Some of our clinicians are also fully qualified musculoskeletal sonographers and will carry out a diagnostic ultrasound scan of your knee.
Many of our clinical specialist physiotherapists are able to perform the scan as part of your assessment (please request when booking if you would like to have diagnostic ultrasound as part of your assessment).

Ultrasound is unable to assess the deep portion of the meniscus, however, it can detect more superficial tears and is also an effective tool to assess for any swelling and inflammation in the knee. Ultrasound can also visualise meniscal cysts and other structures in the knee such as the medial and lateral collateral ligaments and the surrounding tendons. Meniscal cysts are small fluid-filled pockets that arise from the meniscus. These can occur secondary to a tear.
X-Ray
Because a torn meniscus is made of cartilage, it won't show up on x-rays, but it can be helpful to check for any bone damage which might have also occurred with the injury. X-ray is regarded as a gold standard imaging technique capable of accurately diagnosing the presence and severity of bone and joint pathology, including osteoarthritis and broken bones.
How do we treat a meniscal tear?
Meniscal cartilage does not always heal very well once it is torn. This is mainly because it does not have a good blood supply. The outer edge of each meniscus has some blood vessels, but the area in the centre has no direct blood supply. This means that although some small outer tears may heal in time, larger tears, or a tear in the middle, tend not to heal so well. The good news is most of these tears even though they do not heal, become pain and symptom free. This is supported by a significant body of evidence that patients with a meniscus tear in their knee observed on MRI, are often asymptomatic.
At Complete Physio each patient is treated as an individual. Following a comprehensive assessment your physiotherapist will present the best treatment options available to you. Most clients we see with a meniscal tear do improve with a course of physiotherapy, surgery is rare.
The best solution for you will vary depending on your own individual circumstances. There are a number of factors that will determine your treatment:
- Your age
- Your overall health and medical history
- The size and location of the tear
- Your pre injury activity level
- How well you can tolerate specific medications, procedures, and therapies
- The length of time it will take to heal
- Your opinion or preference
Physiotherapy
Most meniscal tears improve with time and physiotherapy. Your Physiotherapist at Complete will provide you with a tailored regime based on your personal profile.
This will often include:
- Activity modification - advice on rest and activity modification allowing the pain to settle.
- Pain management - ice can be effective in reducing pain when applied to the affected area. Some of our physiotherapists may use acupuncture as an adjunct as part of your treatment programme. You may also benefit from taking some anti-inflammatory medication.
- Patient education - it's important to understand your condition and to be active in your recovery. You will be given a clear explanation of the diagnosis and any other underlying causes, and we will discuss what is required to address these issues and reach your goals.
- Range of movement exercises and muscle stretches - your physiotherapist will assess your movement and apply the necessary techniques to normalise your joint and muscle range of movement. You will also likely be given range of movement and stretching exercises to do at home.
- Manual therapy - your physiotherapist may use ‘hands on’, manual therapy such as massage or soft tissue release techniques to the surrounding muscles. This will help improve movement and reduce muscle stiffness or soreness.
- Specific strengthening exercises - with a meniscal tear the muscles around the knee can become weakened increasing the risk of further injury. Your muscles also help to act as shock absorbers; having strong muscles can reduce the amount of stress on your bone and articular cartilage. Your physiotherapist will design a safe resistance program to ensure all your muscle groups are strong and working in synergy, to aid your recovery and prevent recurrence of injury.
- Balance and proprioception - this will involve balance and coordination retraining exercises which will help you return to full function and reduce the chance of reinjury.
- Functional and sports specific training - once your pain, strength, and range of movement improve, functional training can help you safely resume more demanding activities and get you back to playing the sport that you love and minimise your chance of future injury.

Throughout your treatment at Complete Physio, we will keep revisiting your personal goals, so that we maintain the focus on making your life easier and ensuring that you feel supported and involved in your rehab process. We are dedicated to getting you back to full function and we have the correct skills and knowledge within the practice to ensure this goal is achieved.
What if my pain and symptoms don't improve?
Ultrasound Guided Injections
Injection therapy is indicated for a specific group of patients where surgery is not appropriate and pain is limiting the range of movement and function. An injection does not heal the tear but does reduce the pain and inflammation in the joint. An injection can give you a pain-free window to work with your physiotherapist to strengthen the knee and restore the normal mechanics of the joint.
Often the pain associated with a meniscal tear is not coming from the tear itself but inflammation of the joint lining. The lining of the joint is called the synovium. When the synovium becomes inflamed it is called ‘joint synovitis’. Diagnostic ultrasound is the best way of diagnosing synovitis.
At Complete, we will always perform a diagnostic ultrasound of your knee before we consider injection therapy for meniscal tear. This also helps us target the correct area of the knee with an injection. We do not charge extra for the ultrasound prior to injection.
There are two main options; steroid or hyaluronic acid injections.
1) Steroid injection
If pain persists then a steroid injection may be required. A mixture of local anaesthetic and corticosteroid (a potent anti-inflammatory) is injected under the guidance of a real time ultrasound scan. This is to ensure the affected area is accurately targeted. Research has shown that guided injections are more accurate and are more effective at reducing pain than non-guided injections.
2) Hyaluronic Acid injection
Hyaluronic acid is not a drug, it is classified as a medical device. It has no side effects and is an alternative to steroid. It does have anti-inflammatory properties but is not a strong anti-inflammatory like steroid. It works by lubricating the knee joint and improving the shock absorbing properties of the joint. The products we use are called Ostenil Plus and Durolane. These have the highest molecular weight of hyaluronic acid on the market. They are both one off injections.

If you have been diagnosed with a meniscal cyst, an ultrasound guided aspiration and steroid injection can be an effective treatment option. This procedure involves ‘sucking’ the fluid out of the cyst and injecting steroid to stop it returning.
Injection therapy should not be used as a stand-alone treatment. For the best, long-term results it is important that you use the pain relieving effects of the injection to commence a programme of physiotherapy within 2 weeks.
If you would like more information or would like to book an appointment, please contact us on 0207 4823875 or email injections@complete-physio.co.uk.
Surgery for Meniscus Tears
If your meniscal tear causes pain and mechanical symptoms such as clicking, locking or catching, you may require arthroscopic knee surgery. This is performed as a day surgery “key-hole” procedure.
In most circumstances when there is a small tear, the damaged portion of the meniscus is excised. The risk of arthritis in the future can be increased in patients with a meniscal tear who have had a significant portion taken out, especially that of the lateral meniscus which is on the outer part of the knee.
In some circumstances depending on the configuration of the meniscus tear, the tear can be repaired. As the meniscus has a vital role in protecting the articular cartilage within the knee, it is critical that large tears of the meniscus especially in young people are investigated for the possibility of an arthroscopic repair.
At Complete Physio we work with some of London’s most highly regarded and experienced consultants. If an onward referral or surgical opinion is required, we will ensure that you are provided with the best care possible, and will continue to support your recovery every step of the way.
If you would like to book an appointment or speak to one of our expert physiotherapists please call 020 7482 3875 or email info@complete-physio.co.uk.