High Ankle Sprain (Syndesmosis Injury)

Ankle sprains are one of the most common lower leg injuries, but what is the difference between a common ankle sprain and a high ankle sprain?
What is a high ankle sprain (syndesmosis injury)
A high ankle sprain occurs when you tear or damage the high ankle ligaments that connect the tibia to the fibular (lower leg bones). These injuries are much less common than a traditional ankle sprain.
You might hear your high ankle sprain called a “syndesmosis injury”, because this is the name given to the ligaments that are involved in this injury.
Ankle and Lower Leg Anatomy
The ankle joint is composed of a complex hinge joint, with bones, muscles, tendons and ligamentous structures playing a role in its stability.
The ankle joint is formed by three bones in the lower leg: the tibia and fibula (shin bones), and the talus (a small, dome shaped bone in the foot below the tibia). These bones may sustain loads of up to three times a person’s body weight during normal daily activities.
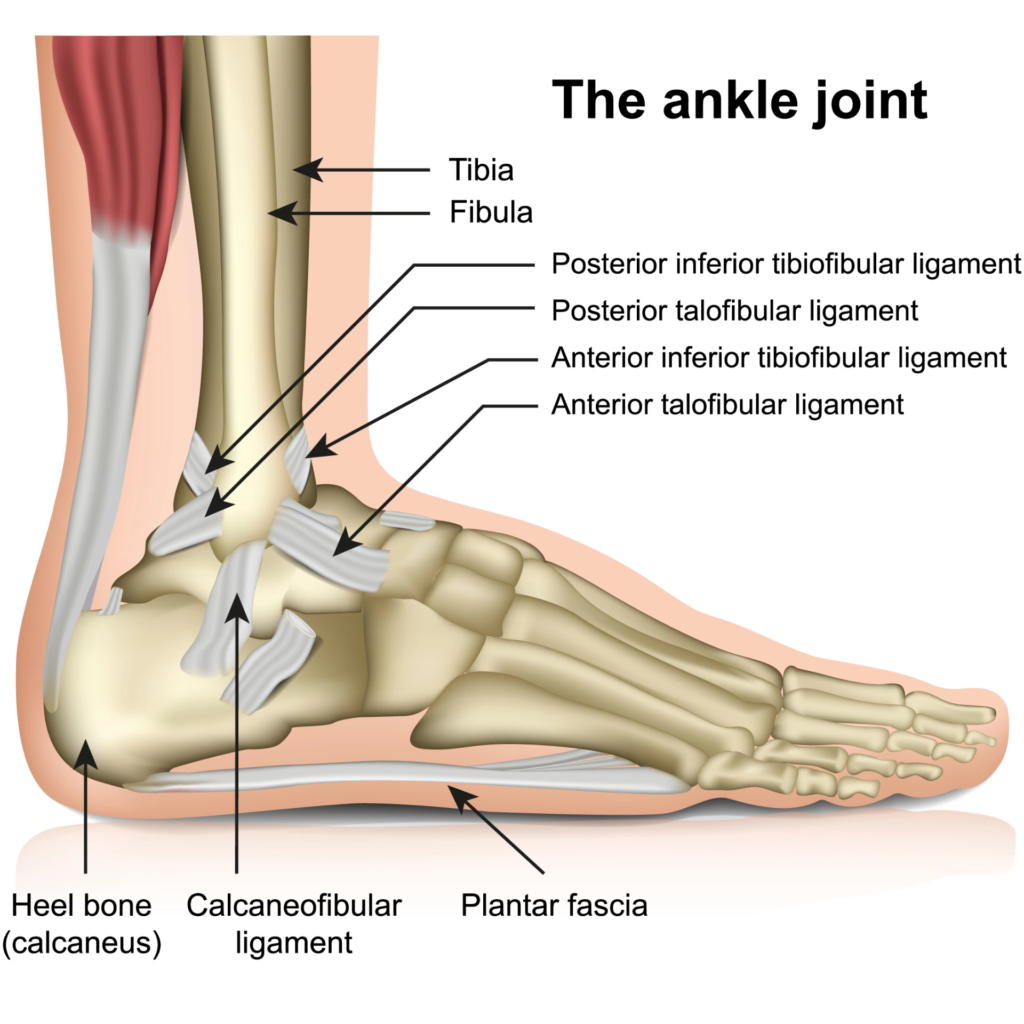
Ligaments are strong, fibrous, soft-tissue bands that connect bones to bones. The ligaments of the ankle allow a wide range of motion while providing stability to the joint.
As well as giving the ankle stability the ligaments provide an even more vital role; over recent years researchers have found that the ankle ligaments contain tiny cells called proprioceptors, these cells provide sensory feedback to the brain, so that your brain knows where your ankle is in relation to your body and to the ground, and what position the ankle is in. Proprioception is closely tied to the control of movement and balance which is essential to help with injury prevention.
The ligaments in the ankle are divided into two groups – the lateral ligaments located on the outside of the ankle, and the medial ligaments located on the inside of the ankle. It is the lower ligaments on the lateral aspect of the ankle that are usually damaged in a common ankle inversion sprain; especially the anterior talofibular ligament (ATFL) as it is the weakest. These ligaments sit across the ankle joint.
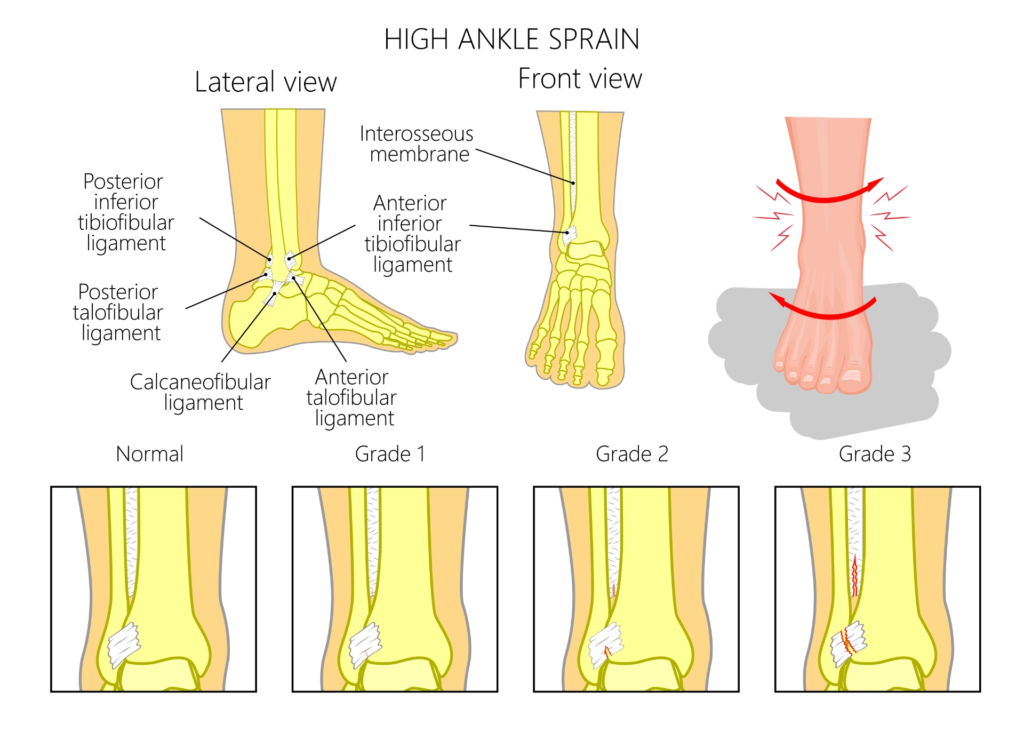
The ligaments that can be damaged or torn in a high ankle sprain include (see above):
- The Anterior Inferior Tibiofibular Ligament (AITFL): found in front of the tibia and fibula.
- The Posterior Inferior Tibiofibular Ligament (PITFL): found at back of the tibia and fibula.
- The Interosseous Membrane: located in the middle space between the two bones.
These ligaments sit just above the ankle joint and any of them can be stretched, torn partially or torn completely in a high ankle sprain.
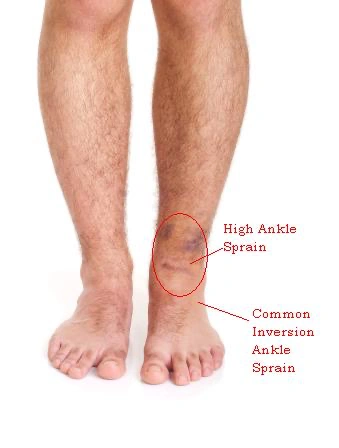
What is the difference between a high ankle sprain (syndesmosis injury) and a low ankle sprain?
As highlighted above, the main difference between a high ankle sprain and a low ankle sprain is the location of the ligament damage, however this is not the only difference.
Most low ankle sprains happen when the ankle rolls, or twists inwards (or sometimes outwards). This usually occurs when stepping off a curb, or walking/running on uneven ground. They are usually low impact, low velocity injuries.
High ankle sprains occur when the foot is forcibly turned outward while your foot is flexed upwards (in dorsiflexion) from either a contact or non-contact injury. They are usually the result of a more sudden, twisting or cutting motion at speed or during a fall or contact sports. It is also a common injury associated with fractures of the distal tibia and fibula.
Low ankle sprains don’t involve the high ankle ligaments, however the lower ankle ligaments are regularly involved in a high ankle sprain, which often results in a delayed diagnosis of a syndesmotic injury.
The key factor between the two is the difference in their management. Delayed or incorrect diagnosis of both low and high ankle sprains can lead to prolonged pain and inability to return to sport.
If high ankle sprains are missed they may require an operation.
Risk Factors
Below are some of the common risk factors for high ankle sprains:
- Flat feet
- A previous injury to the foot/ankle complex
- History of ankle instability
- Participation in contact sports
- Wearing rigid boots such as ski or snowboard boots, or high rugby boots
What are the symptoms of a high ankle sprain (syndesmosis injury)?
Patients with a high ankle sprain without a fracture may be able to weight bear, but will have pain on the outside-front of the leg, over the junction between the tibia and fibula, above the ankle joint level.
This region of pain is higher than with traditional ankle sprains.
Symptoms of a high ankle sprain include:
- Mild/moderate swelling.
- Difficulty bearing weight on the injured leg i.e. limping
- Inability to walk on your toes.
- Bruising on the front, upper ankle that often starts a few days after the injury – this can often be quite mild.
- Pain when pressing on the tibiofibular ligament at the front of the ankle.
- Increased pain when moving the foot up and rotating it to the outside.
How is a high ankle sprain (syndesmosis injury) diagnosed?
Diagnosis can often be delayed because the patient is initially diagnosed and treated for a regular, low ligament ankle injury, and only when the patient fails to improve is a high ankle injury suspected. If it is an isolated high ankle injury, swelling is usually mild or nonexistent and the true nature of the injury can be unappreciated, especially if the joint remains stable.
Our Physiotherapists at Complete are highly skilled in recognising, assessing and diagnosing high ankle sprains. Your physiotherapist will listen to your injury history and your symptoms.
They will also ask questions about your past medical history and gather other relevant information that will help form your diagnosis.
They will then perform a thorough clinical examination to determine the severity of your sprained ankle. It is vital that you get a quick and accurate diagnosis, in order to ensure that you are started on the correct treatment pathway.
If left untreated, your recovery may take considerably longer, and you may end up with recurring ankle problems. In most cases, Complete Physio are able to offer urgent, next day appointments if needed.
Objective Assessment
After your subjective consultation, your Physiotherapist will complete a series of clinical tests and a physical examination, to develop their diagnosis.
Depending on the severity of your symptoms this may include:
- Assessing swelling and bruising.
- Range of movement testing of your foot and ankle.
- Gently palpating (feeling) around the ankle joint and lower leg.
- Measuring the strength, length and flexibility of your lower leg, ankle and foot muscles.
- Looking at functional movements such as squatting, balancing, lunging, stepping.
- Gait (walking or running) analysis.
There are 2 specific tests that your Physio will carry out to assess for a syndesmosis injury:
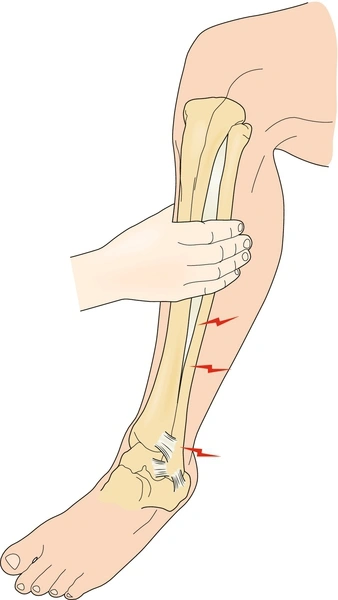
1. The Squeeze Test (see image below)
The therapist will squeeze the lower leg to compress the tibia and fibula. The test is positive if it reproduces symptoms.
2. External Rotation Test (see image below)
The therapist moves the foot into dorsiflexion (pointing upwards) and rotates the lower leg outwards. The test is positive if it reproduces symptoms.

This assessment process is often all that is required to make a diagnosis, however where symptoms are chronic or if the diagnosis is still unclear, your Physio may refer you for additional diagnostic tests such as an X-ray, Ultrasound imaging or MRI.
Diagnostic Ultrasound
The main advantage of diagnostic Ultrasound over an MRI and X – ray is it can dynamically assess the syndesmosis i.e. we can visualise the ligaments whilst moving and stressing the joint.
This provides essential information about the stability of the joint and provides an accurate diagnosis. High ankle sprains with an unstable syndesmosis require a surgical opinion from an orthopaedic foot and ankle specialist.
At Complete Physio, we have a specialist team of clinicians who are dual qualified as both physiotherapists and musculoskeletal sonographers.
We are able to offer patients a unique service that includes both a detailed clinical assessment, and a diagnostic ultrasound scan carried out at your initial Physiotherapy assessment.
X-ray
An X-ray can demonstrate whether there is a fracture (break) in the bone or a widening between the tibia and fibula bones, which might indicate a high ligament injury, however it will not actually show the injured soft tissue, and can therefore cannot rule out a high ankle sprain.
MRI
MRIs are more definitive for syndesmotic injuries. Ruptures of one or more of the ligaments are easily seen on MRI images. If the decision is made to proceed to MRI your physiotherapist can refer you directly.
Please speak to your physiotherapist for more information.
How Is a high ankle sprain (syndesmosis injury) treated?
Treatment depends on severity and an accurate, prompt diagnosis; recovery and rehabilitation may be as short as a few weeks, or as long as six months.
Once your high ankle ligaments are overstretched or ruptured, the bones of your lower leg move apart and you lose a level of your passive ankle stability. It’s crucial to have full stability between the tibia and fibula due to the high forces that pass through the bones when walking and running.
Firstly it is important to determine whether the ankle is stable or unstable. This is usually answered by clinical assessment together with results of the imaging modalities previously described, such as diagnostic ultrasound which can be provided at Complete by our clinical specialists. In the case of suspected complete instability and rupture of multiple ligaments, a referral to a specialist is recommended. Surgery may be needed for severe injuries with notable instability.
Conservative management and rehabilitation of high ankle sprains
Injury Protection and Immobilisation
Unlike the early mobilisation that may be beneficial for a low ankle sprain, many high ankle sprains require a longer period of limited weightbearing with crutches, and may need more substantial bracing or a boot to allow healing.

It is advised at this stage to rest from any movements or activities that cause your pain. You will likely need to stop participating or training for your sport/event for a few weeks.
Pain Relief and Swelling Management
Regular ice with compression and elevation, painkillers and non-steroidal anti-inflammatory drugs, such as ibuprofen, can help you to manage the pain and swelling – please consult your pharmacist or GP before taking any medication.
Range of Movement and Muscle Strength
As your ligaments are healing (up to 6 weeks, but maybe be shorter or longer) they will produce scar tissue. During this time, it is important to maintain soft tissue length and joint range of movement.
You will be prescribed stretching exercises by your physiotherapist to ensure that you optimise your recovery. You also need to be aware that ligaments and soft tissue should not be overstretched, especially in the very early phase of recovery and immobilisation. Your physio will work closely with you to ensure you are happy and confident with the exercises, and your technique is correct.
Your lower leg, ankle and foot muscles will require significant strengthening after a high ankle sprain. It is essential to regain full muscle strength in order to provide excellent, dynamic, ankle control and function.
Your physiotherapist will progress and guide your resistance exercise programme to make certain that you regain your pre-injury strength and power.
During this phase, your physiotherapist may use manual therapy such as massage or soft tissue release techniques to the surrounding muscles, and joint mobilisations. This will help improve joint movement and reduce muscle stiffness or soreness.
Foot and Lower Limb Biomechanics
Your physiotherapist will evaluate your control and movement in your foot and lower leg while you walk and run.
If this is a long-term or recurring issue, you may need a referral to a sports Podiatrist to be assessed for a shoe insert called a foot orthotic and/or exercises to strengthen any weaker muscles, particularly in your calf and feet.
Your physiotherapist may also provide exercises to enhance your walking or running technique.

At Complete Physio we are able to offer an excellent gait analysis service to help evaluate your form and correct any abnormalities. This will not only help your recovery, but also minimise the risk of further injury.
Returning to Sport/Activity

Most high ankle injuries occur during high-speed activities, which place enormous forces on the structures in your ankle
Once your pain settles and you regain full range of movement and strength, you will begin a more complex, customised speed, agility, proprioception and endurance program that will test your ankle and prepare you for sport-specific training.
As mentioned earlier in this article, your ligaments contain tiny cells called proprioceptors, these cells provide sensory feedback to the brain. Balance and proprioception are both adversely affected by injuries such as a sprained ankle. To prevent a recurrence your physiotherapist will guide you through exercises to address these critical components of rehabilitation and improve your sporting performance.

Your physiotherapist will discuss your goals, time frames and training schedules to optimise you for a complete and safe return to sport and at each treatment session they will retest your objective markers, and closely monitor your progress, so that you feel supported throughout your rehabilitation. We are dedicated to getting you back to full activity and function, and helping you minimise your chance for future injury.
Ultrasound-guided Corticosteroid Injection
Corticosteroid is a powerful, injectable anti-inflammatory medication that is routinely used in musculoskeletal medicine to reduce pain and inflammation associated with injury. An injection will only be considered in injuries that have had the assessment including imaging.
Significant research suggests that ultrasound-guided corticosteroid injections are an effective, evidence-based treatment option for persistent pain associated with ankle injuries.
Complete provides a unique injection service run by a team of highly skilled professionals who are fully qualified, independent prescribers, physiotherapists, musculoskeletal sonographers and injection therapists. All injection techniques are performed under ultrasound guidance, as this ensures a more accurate treatment, and has also shown to be less painful, with patients reporting fewer post injection complications.
Cortisone injections shouldn’t be used as a stand alone treatment; they provide a period of pain relief allowing for a ‘window of opportunity’ for you to rehabilitate your ankle effectively. Research has revealed a combination of corticosteroid injection and physiotherapy results in the most successful outcomes; you will likely need to restart your rehabilitation within two weeks after a corticosteroid injection.
We are able to provide a one stop clinic; your clinician will provide an accurate diagnosis, and complete an ultrasound-guided injection, all within the same session. We do not require a GP referral, you can simply self-refer directly into our same day service.
If you would like more information or would like to book an appointment please contact us on 0204 6003994 or email injections@complete-physio.co.uk.
Surgery For a High Ankle Sprain
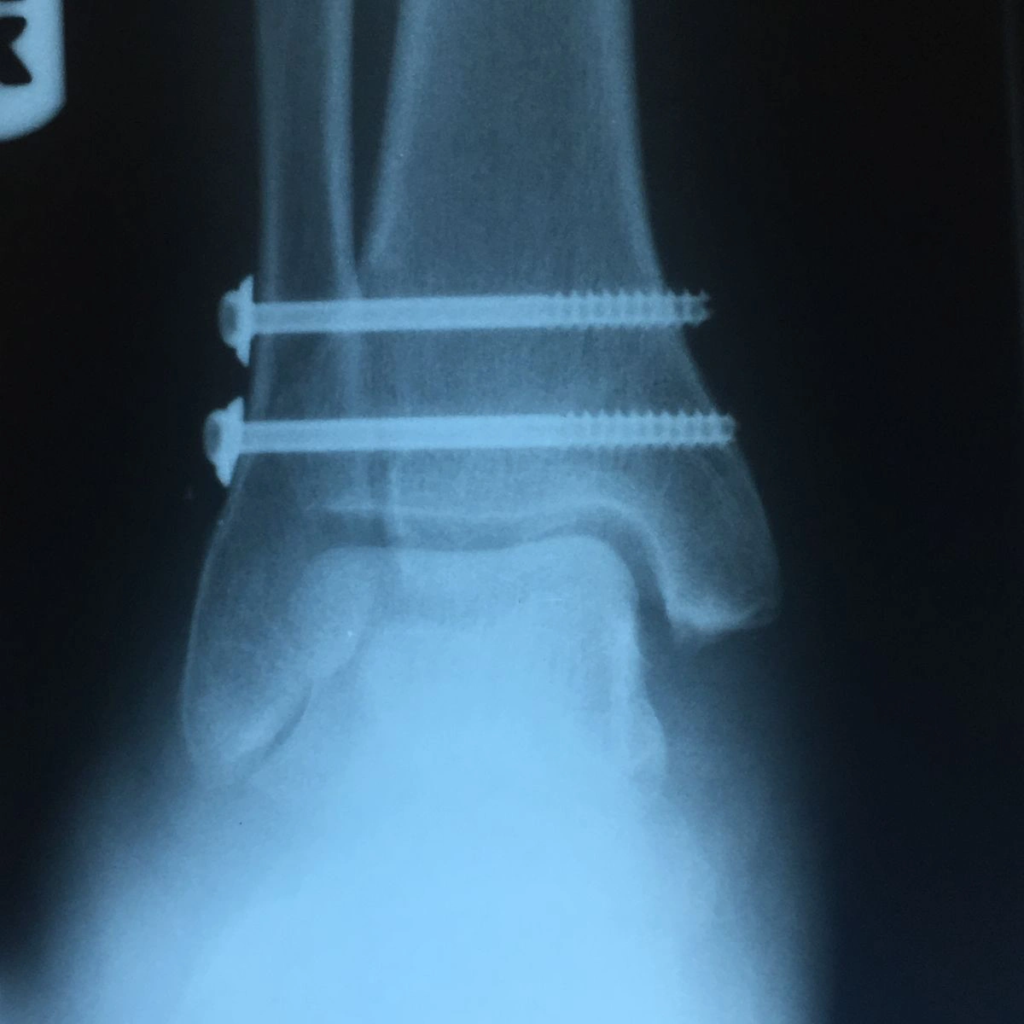
Most high ankle sprains don’t require surgery; however, in severe cases, if a ligament has been completely torn, the standard surgical procedure is to insert a screw between the tibia and fibula to hold the two bones together.
This relieves pressure on the ligaments and allows them to scar in place and heal.
If you do require an onward referral for a surgical opinion, we will ensure that you are seen by one of the highly experienced orthopaedic consultants who we work very closely with, and after surgery you’ll be referred back to your physiotherapist at Complete, to resume another course of post operative rehabilitation.