Vacoped versus Aircast boot – what is the best walking boot following an Achilles rupture?

We are the leading physiotherapy practice in London in the management of Achilles tendon ruptures, whether it is following an operation or if you have been managed nonoperatively.
We are trusted by the top foot and ankle consultants in London to manage their patients following an Achilles rupture. These include recreational and elite/professional athletes from a variety of sports, from Professional footballers to Olympic sprinters.
If you have ruptured your Achilles this article will provide key information around the role and correct use of a walking boot. We also compare the two main walking boots on the market, the Vacoped versus the Aircast boot. For more information visit our YouTube channel where we have several resources to support your recovery.
If you would like to discuss your Achilles rupture with one of our experts, please do not hesitate to contact us on 020 7482 3875 or email info@complete-physio.co.uk.
Introduction
The Achilles tendon is the strongest and largest tendon in the body, but is the most commonly ruptured tendon. Achilles tendon ruptures are on the rise due to an ageing population, obesity and increased sporting activity in the general population.
Traditionally, if you had ruptured your Achilles tendon you would have been managed in a plaster cast and walking using elbow crutches. You were not allowed to put any weight through the injured leg for many months. More recently this has changed and now (whether you have surgery or not) you are encouraged to use a walking boot for a significant period of time during the rehabilitation phase. You are also encouraged from an early stage to start putting weight through the injured limb whilst wearing the walking boot.
Mampal et al 2020, showed that functional rehabilitation with early weightbearing is a safe alternative to traditional immobilising treatment following an Achilles tendon rupture and results in better early functional outcomes.
Valkering et al, 2017, reported enhanced metabolic healing response with functional rehabilitation using a ‘’walking boot’. They also found elevated glutamate levels correlated with increased type-1 collagen synthesis, as well as improved functional outcomes do we need this level of info?
Surgical vs Non Operative (Conservative Treatment) on Achilles Tendon Rupture
There is no clear consensus on the optimal treatment of acute Achilles tendon rupture (ATR). Recent studies have shown the critical role of functional rehabilitation in the treatment of ruptured Achilles tendons.
Non-operative treatment is becoming more common, given the benefits of treating the condition without the risk of complications from surgery. It is also more effective for the NHS to manage a majority of Achilles tendon ruptures conservatively, avoiding the relative expense of surgery. Operative treatment is more prevalent in private practice and in recreational and elite/professional sportsmen. Some consider surgical treatment to be more reliable treatment than conservative treatment for an acute Achilles rupture. For a more detailed review of the pro’s and con’s of surgery and conservative treatment following Achilles tendon rupture read here.
Main concerns of conservative treatment (non -operative treatment)
Traditionally there have been concerns about the conservative (non-surgical management of Achilles tendon ruptures. These concerns included
- Slow rehabilitation
- Difficulty returning to pre-injury activities
- Lower patient satisfaction.
- Longer return to sport
However, recent studies have shown that many of these concerns are not supported by scientific research. Excellent outcomes, with high patient satisfaction, following non-operative treatment using ‘accelerated functional rehabilitation’ have been demonstrated. These have been comparable to the outcomes achieved with operative treatment.
Orthoses - Vacoped vs Air Cast
Whether you have surgery or not, it is likely you will be put in a plaster cast or half plaster cast known as a ‘backslab’ for a few weeks following your injury to ensure the tendon is resting in an optimal position. Following this period you will rely on a cast or a ‘walking boot’ to ensure the tendon heals at the appropriate length.
If you do not have an operation you are relying on the ‘walking boot’ to bring the two ends of the rupture together and optimise the length of the tendon as it heals. If you opt for an operation, your surgeon will bring the two ends of the Achilles tendon together during the operation to optimise tendon length. Following surgery you still need to use a ‘walking boot’ during the rehabilitation phase. This is a key period during your rehabilitation and you must be under the guidance of a physiotherapist with significant experience.
The ’length of the tendon’ is a key factor in successful outcomes.
One of the most important considerations for a successful outcome following an Achilles’ tendon rupture, whether managed conservatively or surgically, is the resultant length of the tendon. The length of the tendon is dictated by the position the foot is in whilst it is healing.
You will generally need to stay in the walking boot for around 8 weeks to maintain this optimal foot position. If the tendon heals in a ‘lengthened’ position due to poor position in the boot or inadequate use of the boot, outcomes will be poor. A lengthened Achilles will result in reduced calf muscle capacity, power and function. Tendons that lengthen in the rehab phase display much poorer reported outcomes. It is thought that up to 10mm of lengthening is tolerable but no more.
‘Equinus’ position
The rehabilitation protocols following an Achilles rupture all insist your ankle joint is held in an equinus position. Equinus essentially means having the foot in a ‘toe pointed’ or what physiotherapists call ‘plantarflexed’ position. Equinus is achieved by using a variety of means, initially a plaster cast and then a ‘walking boot’.
There are two main ‘walking boots’ used in both private practice and NHS. These are the Aircast boot and Vacoped boot. There have been concerns raised that rigid boots with heel wedges such as the Aircast boot do not achieve adequate equinus, resulting in a sub-optimal position and potential tendon lengthening.
What is the Air Cast?
The Air Cast, which includes a wedge kit, allows for a high level of function whilst the Achilles is healing. The Air Cast is easy to use, easy to inflate and to take on and off. Each inflated 'air cell' is easily and quickly customised. It has an enclosed toe cover to protect the foot from hazards and the elements. The tread is durable, gives excellent traction, and absorbs and dissipates energy during heel strike to reduce heel pain.
The Air Cast enables normal walking, reducing forefoot angulation and knee hyper extension. The boot is ventilated and the 'bladders' around the malleoli eliminate pressure sores.

The Aircast boot with wedges
What is the Vacoped?
The Vacoped is a boot that allows for a true equinus position. It is considered to be the gold standard of Achilles tendon orthosis by some foot and ankle consultants. It is more expensive than the Aircast (see later).
It has an adjustable articulating ankle feature, with dynamic settings allowing plantarflexion and controlled range of motion which enables an active recovery. Its vacuum-bead (not sure if this is the right term) forms a strong supportive cast around the foot and ankle, whilst being very comfortable and the external frame enhances that support.

The Vacoped
The Vacoped ROM allows for a patient to walk normally with the boot in-situ and with an ‘Even-up’ shoe. Vacoped is comfortable, custom moulded, has an adjustable range of motion - and is washable & safe to swim in.

Is sufficient ankle equinus (‘toe pointed’) provided by the orthoses?
Do the walking boots we use currently in achilles rehab providing sufficient ankle equinus for optimal healing? Ellison et al (2017) compared the ankle and foot angles in the Aircast boot with wedges and the Vacoped boot:


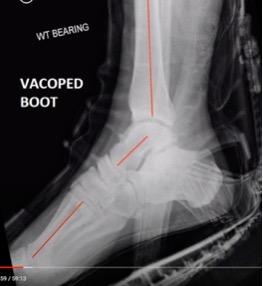
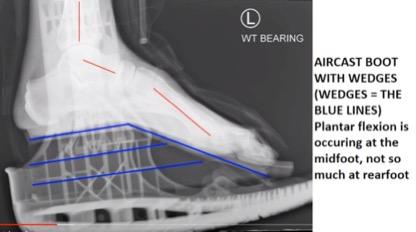
You can see in the picture on the left, of the Aircast boot with wedges, that the appearance of equinus is actually due to the foot bending in the middle, rather than the heel. The picture on the right is the Vacoped boot and you can see that the middle of the foot remains in a straight line, with all the angulation coming from the ankle. This means that whilst the position of both feet looks the same from the outside, when we look at the x-rays we can see that the picture on the left has a lot less ankle plantarflexion (28 degrees) than the picture on the right (48 degrees).
The theoretical concern with these results is that the decreased ankle angle in the Aircast boot will result in poorer outcomes due to increased tendon length. However, there have been no studies investigating this to date. Therefore we cannot say with certainty that this observed difference in ankle angle between the two boots will results in differing outcomes.
Other considerations:
Comfort
The 'no-pressure' Vacoped 'bead liner' guards against pressure sores which improves comfort and therefore less pain. It is also suitable to wear in the swimming pool.
The Air Cast Boot 'bladders' can place pressure on the wound site and can be uncomfortable - so potentially causing pressure sores. The Aircast Boot with wedges also occasionally cause pain at the front of the foot, as the wedges can cause the midfoot to slide down the boot.
Cost
The Vacoped is more expensive.
Vacoped: £300.
Aircast: £150 + £20 (for wedges).
Walking pattern
The Vacoped allows patients to walk in the boot without a limp, being more dynamic.
Waking in the Aircast Boot can cause the patients to be uneven and lurching and can cause unwanted knee and back pain
We also suggest clients use a ‘ Level Up’ to improve the symmetry and comfort of walking in the boot.
Adjustability
Air Cast is easy to fit and use and the wedges are simple to adjust. Adjusting the Vacoped is more complex and this confusion can result in errors when attempting to follow the treatment protocol.
Availability
Vacoped is used in private practices and at some NHS trusts. Many NHS trusts do not use the Vacoped as it is more expensive and does not have clinically proven better outcomes.
The Air Cast is widely used at widely at all private practices and NHS trusts.
Pros vs Cons - Vacoped versus Aircast boot
| Vacoped | Aircast | |
| Cost | £250 | £150 |
| Comfort | +++ | ++ |
| Adjustability | +++ | ++ |
| Gait | More dynamic | Lurching |
| Availability | Limited | Everywhere |
Conclusion
The Vacoped and Aircast with wedges walking boots are both used extensively and successfully in Achilles tendon rupture rehabilitation. There are pro’s and con’s to each boot in regards to comfort, cost and ease of use.
The Vacoped does appear to obtain a more optimal ankle position than the Aircast from the results in the single, small sample study that has been performed. However, there is no evidence currently that this difference in ankle angle results in differing functional outcomes.
If you had ruptured your Achilles tendon it is very important that you see a physiotherapist with extensive experience in managing this condition. Whether you have had an operation or you are being managed non-operatively we have the experience to help you get back to full function as soon as possible.
If you would like to discuss your Achilles rupture with one of our experts or book an appointment, please contact us on 020 7482 3875 or email info@complete-physio.co.uk.