Calcific Tendinitis of the Shoulder
What is Calcific Tendinitis?
Shoulder pain is a common complaint affecting up to a third of the general population, however shoulder calcification is not actually very common. The condition occurs in less than 10% of people being treated for shoulder pain. Unfortunately when it does occur it can be excruciatingly painful.
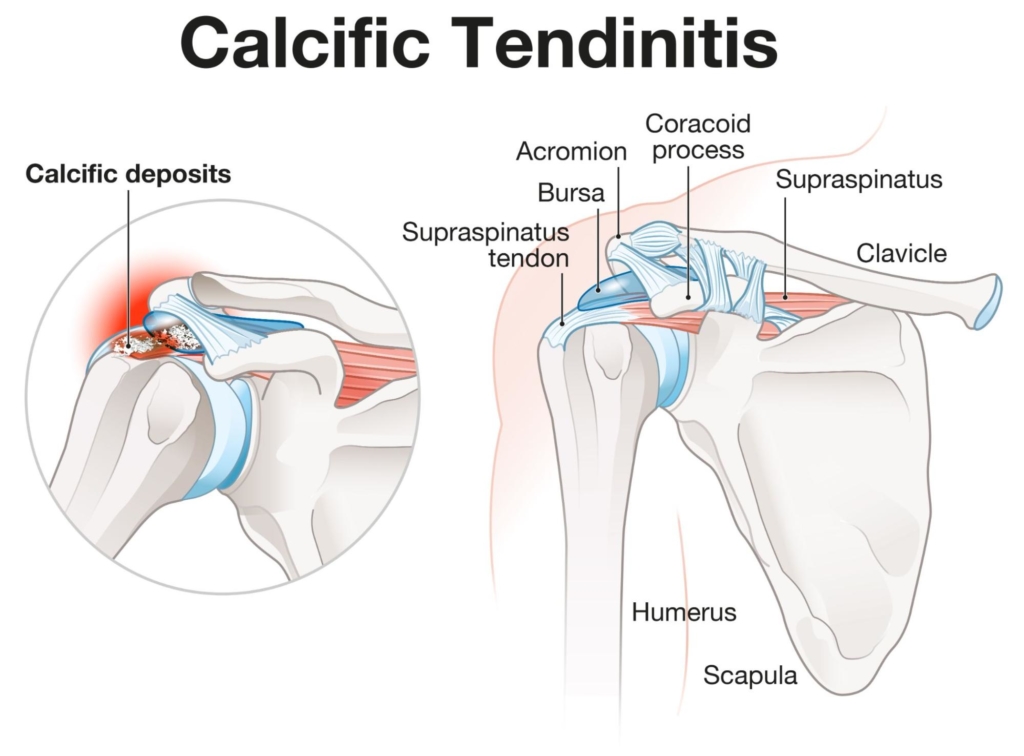
Calcification, or calcific tendinitis of the shoulder, occurs when calcium deposits i.e. bits of bone build up in a rotator cuff tendon. A vast majority of the time the calcium is located in the supraspinatus tendon, but it can also occur in subscapularis and infraspinatus. These calcium deposits vary in size from a few millimetres to a few centimetres. Calcium deposits greater than 1cm often become painful. It is thought that the calcium causes a chemical irritation and build up of pressure in the tendon leading to severe pain.
In addition to the chemical irritation, they are often associated with a very acute subacromial bursitis and/or a shoulder impingement . As the calcific deposits grow bigger, they reduce the space between the rotator cuff and the acromion, as well as affecting the normal function of the rotator cuff muscles. This can lead to subacromial impingement when lifting the arm overhead. This impingement of the rotator cuff tendons will lead to further irritation of the tendon (tendonitis) and subacromial bursa (bursitis), and cause increased pain, making every day life and activities torturous for many patients.
Shoulder Anatomy for Calcific Tendinitis
Your shoulder joint is a ball and socket joint. It is made up of three bones: the upper arm bone (humerus) which is the ‘ball’ (head of humerus), the shoulder blade (scapula) which is the ‘socket’ (glenoid), and the collarbone (clavicle). Your arm is kept in the shoulder socket by the rotator cuff muscles.
The rotator cuff consists of four tendons: supraspinatus, subscapularis, infraspinatus, and teres minor. The role of the rotator cuff is to provide stability to the shoulder joint and help to produce movement such as lifting and rotating the arm. The most commonly affected tendon is the supraspinatus tendon.
There is a thin sac called a bursa located between the rotator cuff and bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm. If the calcium deposits lead to shoulder impingement, this can cause the bursa to become inflamed.
What causes calcific tendinitis?
The cause of calcium deposits within the rotator cuff tendon is not entirely understood. It is thought to be related to wear and tear of the tendons, and a dysfunction in the normal healing process. It tends to affect people between the ages of 40 and 60 and women are slightly more likely to be affected than men.
There is also some suggestion that hormone problems such as thyroid abnormalities and metabolic conditions such as diabetes may be a risk factor
There are four stages to the formation of calcification:
- Pre-Calcification stage - In this phase, the calcification site starts to undergo cellular changes that put the tissues at risk of developing calcium deposits. This is usually a non-symptomatic stage i.e. there is no pain at this stage, so you will not know it is occuring.
- Calcific stage - The calcium is excreted from cells during this stage and then blends into chalk like calcium deposits. Once the calcification has formed, a so-called, pain free, resting phase begins.
- Resorptive stage - This is also known as the painful stage. After the resting phase, a resorptive phase begins; the calcium deposits begin to change into a toothpaste (softer) type substance, causing increased pressure and swelling within the tendon and triggering significant inflammation and pain. This is often when the pain can be excruciating and it is not uncommon for patients suffering with acute calcific tendinitis to attend A&E due to the severity of the pain. During this phase conservative treatment including non-steroidal medication such as Ibuprofen can be ineffective and an ultrasound guided steroid injection should be considered.
- Post-Calcific stage - During the post calcific phase, the calcific deposits within the tendon are reabsorbed by the model during a process called remodelling and often disappear. This can take many months/years to complete; as the calcium deposits slowly disappear and are replaced by more normal tissue. This phase is often less painful or pain free.
Although these stages are well documented, the condition does not always follow these specific stages. The length of time each stage lasts can also vary.
What are the symptoms of calcific tendinitis?
The clinical picture may vary from patient to patient, depending upon which phase the deposit is in, but pain is certainly the hallmark of this condition.
Common symptoms of Calcific Tendinitis
- Acute/severe pain located at the side of your shoulder which may refer down towards the elbow.
- Sudden or gradual onset of pain (as the calcium deposits build up)
- Increased pain lifting your arm, especially overhead or away from the body.
- Pain that is worse at night. This may affect your ability to go to sleep or wake you up.
- Sensations of weakness in your arm.
- Pain when lifting or carrying objects such as shopping bags.
If you are experiencing any of these symptoms, or suspect that you have an acromioclavicular joint injury, and would like to see one of our expert physiotherapists you can call 0207 482 3875 or email info@complete-physio.co.uk. If you would like to speak to a specialist before booking, then please send us an email with your details and we will call you back.
How is calcific tendinitis diagnosed?
Your Physiotherapist at Complete can provide a clinical diagnosis of shoulder impingement syndrome however, a clinical assessment alone is not able to reliably diagnose calcium within the tendon,
A diagnostic ultrasound scan is required to obtain a full and accurate diagnosis of the cause of your shoulder pain. Obtaining a correct diagnosis is essential, allowing for the most appropriate and effective treatment strategy to be implemented. At Complete Physio only our clinical specialist physiotherapists carry out diagnostic ultrasound scans. Please make it clear if you require an ultrasound scan at the time of booking.
Diagnostic ultrasound for Calcific Tendinitis
Diagnostic ultrasound imaging is the most sensitive imaging technique to diagnose calcific tendinitis (Image 1). Diagnostic ultrasound scans are more accurate than magnetic resonance imaging (MRI) in the diagnosis of calcium deposits within the tendon (Image 2). Ultrasound can also provide valuable information regarding the specific stage of the calcific deposit. Diagnostic ultrasound has also been proven to be excellent at visualising inflammation associated with tendon and bursa. It also has the unique ability to dynamically assess the movement of the tendon in real-time, not possible with MRI.
The calcific deposit can be seen on plain x-rays (Image 3). Diagnostic ultrasound scan is better to find small calcific deposits which can be missed on x-rays and MRI. Ultrasound also makes it possible to assess the size of the deposit in all directions which cannot be achieved with x-ray.
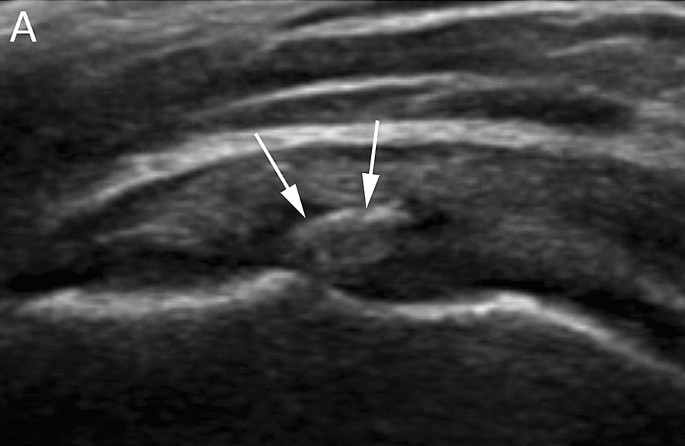
An ultrasound scan of a small calcific deposit in supraspinatus tendon
At Complete Physio our clinical specialists carry out an ultrasound scan as part of their clinical assessment. The combination of the physical examination and ultrasound will help determine the provision of an evidence-based treatment program to relieve your symptoms and allow you to return to the activities you enjoy.
We do not charge extra for an ultrasound scan, and you do not require a GP referral. If you would like to book a physiotherapy appointment, including an ultrasound scan, please ensure you inform our administration team. Please inform our administration team if you require an ultrasound scan at your appointment to ensure you see the correct clinician.
If you would like to discuss your shoulder pain before booking or are not sure whether you should have a scan, please call 020 7482 3875 or email info@complete-physio.co.uk and one of our specialists will contact you to discuss.
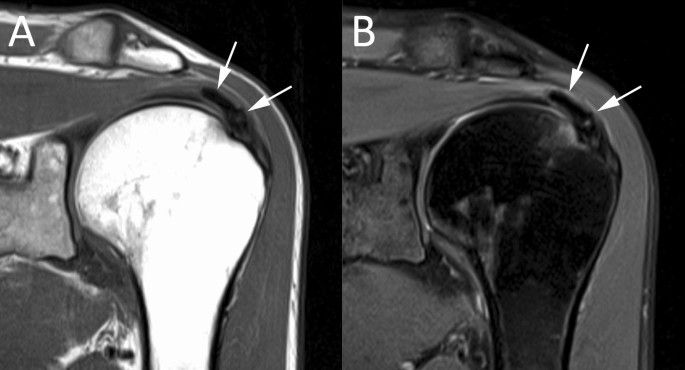
Albano et al 2020 - An MRI scan of a calcific deposit in supraspinatus tendon. MRI is less sensitive than an ultrasound scan for identifying calcium within the rotator cuff

An X-ray of a calcific deposit in supraspinatus tendon. X-rays are less sensitive than an ultrasound scan for identifying calcium within the rotator cuff.
How do we Treat Calcific tendinitis?
The main goal of any treatment is to reduce the pain and inflammation in the shoulder joint, and restore normal movement and function. A majority of calcific tendinitis are self-limiting and will resolve with a period of rest, physiotherapy, and a short course of non-steroidal medication. For those that do not settle, an ultrasound guided injection should be the next step.
Anti-inflammatory medications for Calcific Tendinitis
These medications can be helpful in reducing swelling or inflammation in the shoulder joint, there in turn reducing pain. These should be used under the guidance of a GP or specialist clinician.
Physiotherapy for calcific tendinitis
At Complete Physio, our clinicians are experts in the diagnosis and management of shoulder pain. Physiotherapy is designed to improve your quality of life through hands-on care, patient education, and prescribed movement and exercise. Initially, physiotherapy will focus on reducing the pain and inflammation, it will also involve a combination of corrective strengthening and stretching rehabilitation exercises, manual techniques including massage and soft tissue release, and postural advice. Our goal is to get you back to full function as quickly as possible.
Your physiotherapy treatment will aim to:
- Reduce pain and inflammation
- Normalise joint range of motion
- Improve your shoulder blade and shoulder alignment and scapular control
- Normalise your muscle lengths
- Regain full muscle strength throughout the shoulder, especially the rotator cuff muscles
- Improve your technique and function, e.g. lifting and overhead activities.
- Restore High Speed, Power, Proprioception & Agility
- Minimise your chance of re-injury as you return to sport or work.
Your physiotherapist at Complete will provide you with a tailored regime based on your personal profile. This will often include
- Pain management - This may include applying ice to the affected area and ensuring that you get adequate pain relief via your GP and pharmacist .If the pain is very severe and acute, we may suggest you wear a sling for a few days to allow the pain to settle down. We will also discuss the role of an ultrasound guided steroid injection (also known as a cortisone injection) to settle down the pain. This will be discussed in more detail later in this article.
- Patient education - one of the most important and effective aspects of rehabilitation is to understand more about the problem and the best ways to facilitate and take part in your own recovery. You will be given a clear explanation of the diagnosis and any other underlying causes, and we will discuss what is required to address these issues and reach your goals.
- Range-of-movement exercise - Your physiotherapist may teach you self-stretching methods and some gentle exercises to decrease tension, muscle spasm and help restore normal motion of your shoulder.
- Manual therapy - these techniques help to improve movement. Your physiotherapist may use manual therapy to help guide your shoulder into a less stressful or painful movement pattern. It may also include some soft tissue release techniques to the surrounding muscles.
- Muscle strength - muscle weaknesses or imbalances can cause or contribute to impingement problems of the shoulder. Your physiotherapist will design a strength programme for the muscles surrounding your shoulder. This part of your treatment will be very closely monitored to ensure that you are not causing any further damage to the injured tendon. You will work on both the smaller, stabilising, rotator cuff muscles, as well as the bigger, more global muscles in the whole of the upper limb, back and neck. If pain is limiting your ability to engage in physiotherapy, an ultrasound guided steroid injection should be considered to provide pain relief to be able to carry out the exercise more effectively.
- Functional and sports specific training - Once your pain, strength, and range of movement improve, functional training can help you safely resume more demanding activities and get you back to work, or playing the sport that you love.
Throughout your treatment at Complete Physio, we will keep revisiting your personal goals, so that we maintain the focus on making your life easier and ensuring that you feel supported and involved in your rehab process. We are dedicated to getting you back to full function and we have the correct skills and knowledge within the practice to ensure this goal is achieved.
Shockwave treatment for calcific tendinitis
Shockwave therapy is used to stimulate tendon healing and can be an effective treatment for breaking down the calcium deposits. It is not an appropriate treatment if you are in the resorptive painful stage. However, it is appropriate once the acute pain has reduced and is under control.
Shockwave produces powerful sound waves that create an environment of controlled microtrauma to the region. This directly targets the calcium within the tendon.
Evidence has revealed that shockwave therapy:
- stimulates a healing response
- causes fragmentation of calcium deposits within a tendon
- encourages reabsorption of the calcium by the body
- reduces pain by desensitising local nerve endings
A course of 3 to 6 treatment sessions are required. This should be accompanied by a course of physiotherapy for optimum results.
For more information about shockwave therapy for calcific tendinitis click here.
At Complete Physio, we carry out Shockwave at four of our conveniently located sites.
Steroid Injections for calcific tendinitis
Ultrasound guided injection therapy is an accurate and effective treatment technique used to reduce pain and increased movement. Steroid, also known as cortisone, is a very powerful steroid and can be very effective at easing inflammation and swelling. Usually, for calcific tendinitis, an injection of steroid into the inflamed bursa (known as subacromial bursitis) above the calcium deposits significantly improves pain. It is essential to use ultrasound to direct the steroid into the right region. A single injection provides rapid pain relief and allows a window of opportunity to maximise the benefits of your physiotherapy rehab.
At Complete Physio, we carry out both shockwave and ultrasound guided injections at four of our conveniently located sites.
“Barbotage & Lavage” injection for calcific tendinitis
There is a specific, advanced injection technique that we carry out at Complete for calcific tendinitis called a “barbotage and lavage procedure”. “Barbotage & lavage” is a technique involving the use of both local anaesthetic and corticosteroid. After using a local anaesthetic, a needle is used to break down and suck out the calcium deposits. Generally, the aim is to remove or break down most of the calcification; this helps the body to reabsorb it. You may need more than one treatment, however, evidence does suggest that the “barbotage and lavage” injection procedure for calcification is as effective as surgery.
This procedure often results in a dramatic reduction in the patient’s pain symptoms. We also provide a graded exercise program to follow in order to help the shoulder return to normal strength and function in the days after the injection procedure.
At Complete Physio, we carry out these ultrasound guided injections at four of our conveniently located sites.
Surgery for calcific tendinitis
In general, surgery for calcific tendonitis is reserved for cases that fail other treatments. Most doctors agree that surgery should only be considered after six months. Surgery involves removing the calcium deposits and opening the space between the shoulder tendons and bone. Care is taken to ensure that the calcium has been completely removed by doing an x-ray at the end of the procedure.
If you would like to book an appointment or would like more information before booking please call 020 7482 3875 or email info@complete-physio.co.uk