What is shoulder impingement, bursitis, and tendonitis?
The shoulder is a complex joint made up of many muscles and tendons that allow a great range of movement in your arm. This makes it vulnerable to many different problems, so, it is no surprise that it is often a source of pain and discomfort for many people. In fact, shoulder pain is one of the most common injuries we treat at the clinic.
Shoulder impingement (also known as shoulder impingement syndrome (SIS) is a frequent cause of shoulder pain. Shoulder impingement has been reported to be the main contributing factor in over 65% of all patients suffering from shoulder pain.
It is a term that is used to describe several conditions The two main structures involved are:
1/ Shoulder subacromial bursitis - occurs when the bursa becomes inflamed and swollen, this is known as a bursitis i.e., inflammation of the bursa, The bursa is a thin, fluid-filled sac located between the rotator cuff tendons and the deltoid muscle in the shoulder). A normal bursa is a thin layer of tissue, designed to allow friction free movement between the tendon and the muscle. A bursitis can cause a sharp, acute pain with certain movements, followed by an achy pain that can travel down the arm. It is not uncommon for a bursitis to cause pain at night.
2/ Rotator cuff tendonitis (also known as tendinopathy) - occurs when the rotator cuff tendons become irritated, damaged, or worn down. The rotator cuff tendons swell and cause pain in the shoulder and can also cause pain in the upper arm.
Impingement syndrome is a descriptive term for pain arising from the tendons and bursa in the shoulder.
Shoulder impingement occurs when there is inflammation of the rotator cuff tendons and/or the bursa. There is a difference between tendonitis and bursitis, but there is usually a combination of these problems in most cases.
Shoulder Anatomy
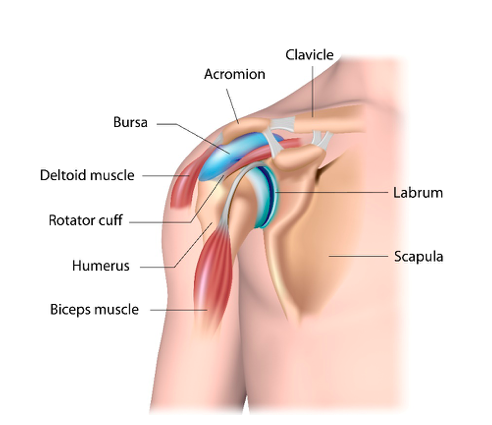
Your shoulder joint is a ball and socket joint. It is made up of three bones: the upper arm bone (humerus) which is the ‘ball’ (head of humerus), the shoulder blade (scapula) which is the ‘socket’ (glenoid), and the collarbone (clavicle).
Your arm is kept in the shoulder socket by the rotator cuff muscles. The rotator cuff consists of four tendons: supraspinatus, subscapularis, infraspinatus, and teres minor. The role of the rotator cuff is to provide stability to the shoulder joint and help to produce movement such as lifting and rotating the arm. The most common tendon injured is the supraspinatus tendon.
There is a thin sac called a bursa located between the rotator cuff and the deltoid and bone on top of your shoulder (acromion). The bursa allows the rotator cuff tendons to glide freely when you move your arm.
What causes shoulder impingement?
Under normal conditions the tendons slide effortlessly within the sub-acromial joint space (the space between the acromion and the humerus) allowing for smooth, pain-free movement. However, if there is an injury which causes inflammation of the tendons and/or bursa they can swell and take up more of the space. Once this has occurred the problem can be self-exacerbating and can take time to settle down. Inflammation causes a thickening of the tendons and bursa. The thickening then takes up more space, and the tendons and bursa can become pinched and inflamed, and so on. This is often referred to as secondary impingement.
Alternatively, in some individuals the subacromial space becomes too narrow due to structural or bony changes of the joint. This causes irritation to the tendons and bursa, which become inflamed. Inflammation causes the tendons and bursa to swell, making the space for movement still smaller. Eventually, every time they move their arm, the tendons and bursa are pinched between the bones. This is known as primary impingement.
Repeated, minor trauma of the shoulder joint and muscles or a single more significant injury such as a fall are the most common causes of bursitis and tendonitis.
Main causes/contributing factors include:
Athletes – people who participate in sports that involve the repetitive use of the shoulder or overhead activity (swimmers, tennis players, cricketers, throwers, etc.), are more susceptible to shoulder impingement
Age - most patients with this condition are between 40 and 65yrs old. As we age, our muscles and tendons can be worn down or weakened, making them more prone to injury and inflammation. Older people can also develop extra ridges of bone in the shoulder. These ‘bony spurs’ can cause impingement on the tendons or bursa, by narrowing the sub-acromial joint space
Anatomy – there is natural variation in the shape of our arm bones and shoulder blades. Some people have a tighter sub-acromial space in their shoulder and may be more prone to impingement.
Posture - with modern lifestyles, ageing and injury, many of us adopt unhelpful or abnormal postures causing our shoulder blades and shoulder joint to sit and move incorrectly. This increases our risk of shoulder pain.
Muscle weakness or imbalance - we can develop strength and control deficits in our rotator cuff muscles that can provoke symptoms of impingement. For example, it is not uncommon that patients have weak rotators of the shoulder. Even muscles in other parts of the body can affect the shoulder joint. It is common to discover subtle weaknesses in core stability or the legs of patients with shoulder pain.
Trauma - it can also begin after a fall, from lifting or carrying something too heavy or from unaccustomed activity, for example playing tennis for the first time for a few years. This can cause inflammation of the tendons and/or bursa.
Occupation - those who do repetitive lifting or overhead activities using the arm, such as wallpaper hanging, construction, or painting are also susceptible.
Medical conditions – bursitis and tendonitis are also associated with other problems such as arthritis, gout, diabetes, and thyroid disease.
Infection - may also cause it, although this is less common.
What are the symptoms of shoulder impingement?
Patients with rotator cuff symptoms and/or sub-acromial bursitis usually present with pain located on the side of the upper arm and weakness in the shoulder. The pain is often a dull ache (like toothache) with a sharp pain when performing certain movements. This can be a very painful condition, particularly at night if you lie on it. Patients often have difficulty lifting their arm, putting their hand behind their back, during overhead activities such as playing tennis, and lifting weights in the gym.
Common signs of shoulder impingement include:
- Pain over the outside of the shoulder/upper arm, sometimes radiating down the arm towards the elbow.
- Sharp, more intense pain with overhead activities such as washing hair and reaching into high cupboards
- Unable to lie on the painful shoulder
- Often the pain will keep you awake at night
- Loss of arm strength
- Painful arc of movement – shoulder pain felt between 60 – 90° of the arm moving up and outwards.
If you are experiencing any of these symptoms, or suspect that you have a shoulder impingement, and would like to see one of our expert Physiotherapists you can call 0207 482 3875 or email info@complete-physio.co.uk. If you would like to speak to a specialist before booking, then please send us an email with your details and we will call you back.
How is shoulder impingement diagnosed?
Having discussed your symptoms and the history of your injury and pain, your skilled shoulder physiotherapist will diagnose your shoulder impingement during a clinical examination. They will perform a series of specific shoulder impingement tests. They will also check for signs of tenderness or deformity, assess for shoulder range of motion and rotator cuff strength. They will look at your posture and scapular positioning and its influence on the impingement and perform any other appropriate tests.
The main elements of a physical assessment include:
- Postural assessment of your shoulder joint, shoulder blade and spine.
- Shoulder range of movement tests
- Rotator cuff strength tests.
- Shoulder impingement tests – a series of specific tests designed to reveal the presence of shoulder impingement. This can be somewhat uncomfortable; however, it is an essential part of the clinical assessment.
- Palpation (feeling) structures within the shoulder to locate the source of the symptoms.
- Functional tests - if your pain is present during a specific activity or task, you may be asked to perform these, so the physiotherapist can assess exactly what is aggravating your pain.
Diagnostic ultrasound may be required to confirm an accurate diagnosis and pinpoint the direct cause of your shoulder pain. Obtaining a correct diagnosis is critical, allowing for the most appropriate and effective treatment strategy to be selected for you.
Diagnostic Ultrasound Scan
An ultrasound scan is a very sensitive imaging modality for diagnosing the root cause of your shoulder impingement. Ultrasound is a cost effective and highly accurate diagnostic test. The scan will assess your rotator cuff tendons and bursa and other structures of the shoulder. The scan will also reveal if there is a tear in the rotator cuff tendons. During your diagnostic ultrasound scan, your clinician will ask you to move to assess what is happening as your shoulder moves through the painful region. This can provide essential information to ensure we obtain the correct diagnosis.
The combination of the physical examination will help determine the provision of an evidence-based treatment program to help relieve your symptoms and allow you to return to the activities you enjoy.
At Complete our clinical specialists carry out an ultrasound scan as part of their clinical assessment. We do not charge extra for an ultrasound scan, and you do not require a GP referral. If you would like to book an appointment including an ultrasound scan, please ensure you inform our administration team.
MRI Scan
An MRI scan is not required for a majority of impingement type symptoms. Shoulder impingement is unlikely to be viewed on MRI. MRI is a static test performed in a non-impingement zone, e.g., arm by your side. An MRI is used for patients with an unstable shoulder, for example following a shoulder dislocation. An MRI visualises the deeper structures in the joint better than ultrasound, such as the articular cartilage on the humerus i.e., the “ball” of the “ball and socket”. It also visualises the labrum, which is the cartilage attached the “socket” of the joint, known as the glenoid labrum.
X-Rays
X-rays do not show impingement but do show the shapes of the bone and can show whether there are any bony spurs or breaks in the bone. It can also show if you have a narrow subacromial space. For most impingement problems an X-ray has limited use.
Your specialist at Complete Physio will guide you on the most appropriate clinical and diagnostic tests and refer you to an appropriate consultant if further investigations are required.
How do we treat shoulder impingement?
Shoulder impingement may irritate numerous structures of the shoulder. Each structure may require a different treatment modality. Understanding why the impingement has occurred in the first place is the most important step to both the short-term resolution and the prevention of recurrent problems. Most patients suffering with shoulder impingement syndrome respond positively to physiotherapy treatment.
Researchers have concluded that there are seven stages that need to be covered to rehabilitate shoulder impingement and prevent recurrence effectively.
These are:
- Early injury management - protection, pain relief & anti-inflammatory treatment
- Improve shoulder range of movement
- Restore scapular (shoulder blade) control and scapulohumeral rhythm – the relationship between the shoulder blade and the upper arm movement.
- Regain normal neck, shoulder blade, spine, and shoulder posture and function.
- Regain full muscle strength – specifically rotator cuff muscles, but also more global and core muscle strength
- Restore high speed, power, proprioception of the shoulder and upper limb
- Return to sport or work
Conservative treatment will be managed by your physiotherapist and often includes the following modalities:
- Education and advice - one of the most important and effective aspects of rehabilitation is to understand more about the problem and the best ways to facilitate and take part in your own recovery. You will be given a clear explanation of the diagnosis and any other underlying causes, and we will discuss what is required to address these issues and reach your goals.
- Activity modification, posture re-education and ergonomic advice to help allow your pain and symptoms to settle.
- Manual therapy - including joint mobilisations or manipulations and soft tissue techniques such as massage.
- Range of movement exercises for your shoulder and neck.
- Specific strengthening exercises for the muscles surrounding your shoulder.
- Targeted stretching and manipulation for any tight muscles.
- The application of corrective physiotherapy tape - this is used to help correct shoulder position and allow a reduction in pain during movement.
- Upper limb proprioception exercises
- Functional and sports specific exercises.
Shoulder Impingement Exercises
Due to the large variability between patients who experience shoulder impingement, each patient must receive a customised shoulder impingement exercise program. It makes sense that a swimmer suffering from a swimmer’s shoulder would receive a different exercise regime than a tennis player or an elderly lady who merely wishes to reach overhead to open a cupboard or hang their washing.
Your physiotherapist at Complete will work closely with you to ensure that your treatment is tailored to your specific needs. We will keep revisiting your personal goals, so that we maintain the focus on making your life easier and ensuring that you feel supported and involved in your rehab process. We are dedicated to getting you back to full function and we have the correct skills and knowledge within the practice to ensure this goal is achieved.
When are Corticosteroid Injections Helpful?
Steroid injections may be helpful in the initial pain-relieving stage when acute shoulder bursitis/tendonitis occurs, particularly if you have pain waking you at night. It may also be considered if your symptoms are not resolving following a complete course of physiotherapy rehabilitation.
Under ultrasound guidance, the corticosteroid (also known as steroid), is given directly into the bursa above the rotator cuff tendons. The injection can have a fast-acting effect, significantly reducing pain, irritation, and inflammation of the bursa. The purpose of this is to then allow you to fully rehabilitate the shoulder.
No injection should be considered as a standalone treatment. Research has shown significantly better outcomes when injection therapy is combined with physiotherapy rehabilitation and therefore, Complete highly recommend you start a course of physiotherapy within 2 weeks after receiving an injection. If you would like more information or would like to book an appointment, please contact us on 0207 4823875 or email info@complete-physio.co.uk.
Surgery
Surgery is sometimes recommended for shoulder impingement if symptoms do not settle following a course of physiotherapy. If this is required, your physiotherapist will be able to refer you to the correct consultant, to ensure you get the best possible care and outcome.
A physiotherapy guided rehabilitation programme will be needed following surgery to restore the full range of movement to your shoulder.
At Complete Physio we provide a comprehensive, “one stop clinic” for shoulder impingement, from diagnosis to treatment, including ultrasound guided injections. All these treatments can be carried out within our London clinics, which means you don’t need to visit different specialists. Our “one stop service” also makes your treatment more affordable and accessible. If you would like to discuss your treatment before booking in, please do not hesitate to contact us, and one of our expert physiotherapists will call you back.
To make an appointment please email info@complete-physio.co.uk or call 020 7482 3875.