Why do I get shoulder pain when I serve?

Every year, tennis fever grips the nation, with more and more people rallying to pick up their racquets, get on court and channel their inner champion.
It is estimated that over 20% of the nation’s tennis participants are based in London. As such, at Complete Physio we see a number of clients presenting with tennis related injuries.
Studies suggest that shoulder pain can occur in 25 – 50% of tennis players, depending on their age and level of participation. In this post, we aim to identify why these injuries can occur and what to do if you develop symptoms.
Anatomy of the shoulder
To understand shoulder injuries, it is important to first consider the anatomy of the shoulder and how it relates to its function.
First and foremost, the shoulder is a complex anatomical region that involves not one, but four joints that interact to allow movement of the arm. The shoulder is therefore better referred to as the “shoulder girdle”, rather than a joint. The 4 joints that make up the shoulder girdle are:
- The Glenohumeral joint
- The Acromioclavicular joint
- The Sternoclavicular joint
- The Scapulothoracic joint

Each of these joints are structured to allow interaction and a wide range of motion for the shoulder to move. As a result, the shoulder girdle is the most mobile region of the human body and relies on muscular rather than ligamentous structures for its integrity. Whilst this structural make up allows for great movement control and precision at the shoulder, it also means that it is more susceptible to injury.
Among the structures associated with the shoulder girdle are tendons, bursae and the labrum. Tendons are cord-like structures that connect muscle to bone, such as biceps and the rotator cuff tendons illustrated below.
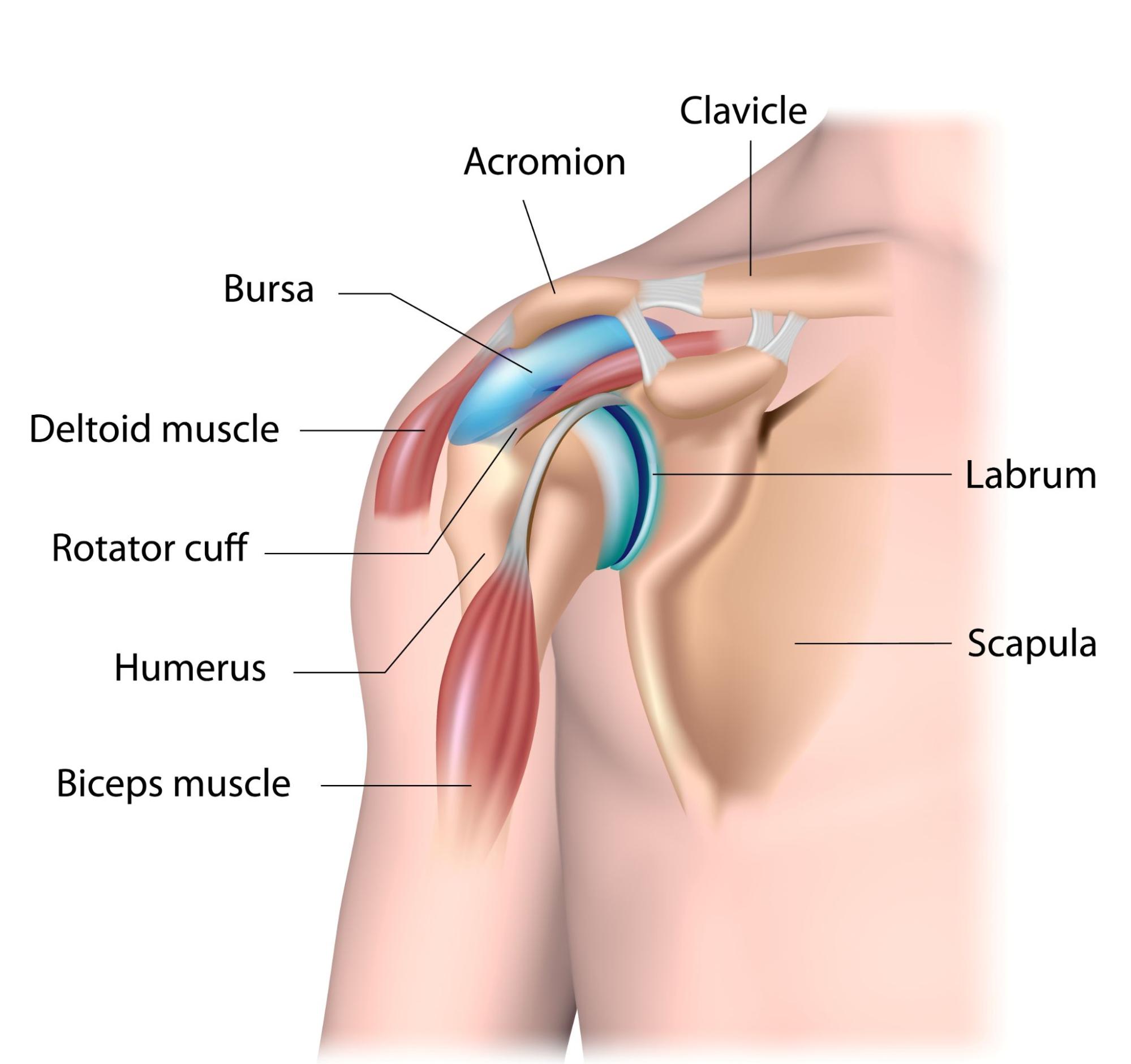
Bursae are fluid-filled sacs that offer cushioning and lubrication between muscles, ligaments and bony prominences. Finally, the labrum is a cartilage that forms a rim around the glenoid to accentuate the socket shape of the joint.
Tennis Injuries

Whilst taking part in sporting activities is considered good for your health, there are times when injuries can occur. Among the common injury sites in tennis is the shoulder, of which a common problem is shoulder impingement.
Shoulder impingement is an umbrella term for an array of injuries that occur at the shoulder, including:
- an inflammation of the long head of biceps tendon.
- Sub-acromial bursitis – an inflammation of the bursa that sits between the acromion and head of the humerus
- Rotator cuff pain – most commonly caused by an inflammation of the rotator cuff tendons, or in some cases a tear in the muscle or tendon.
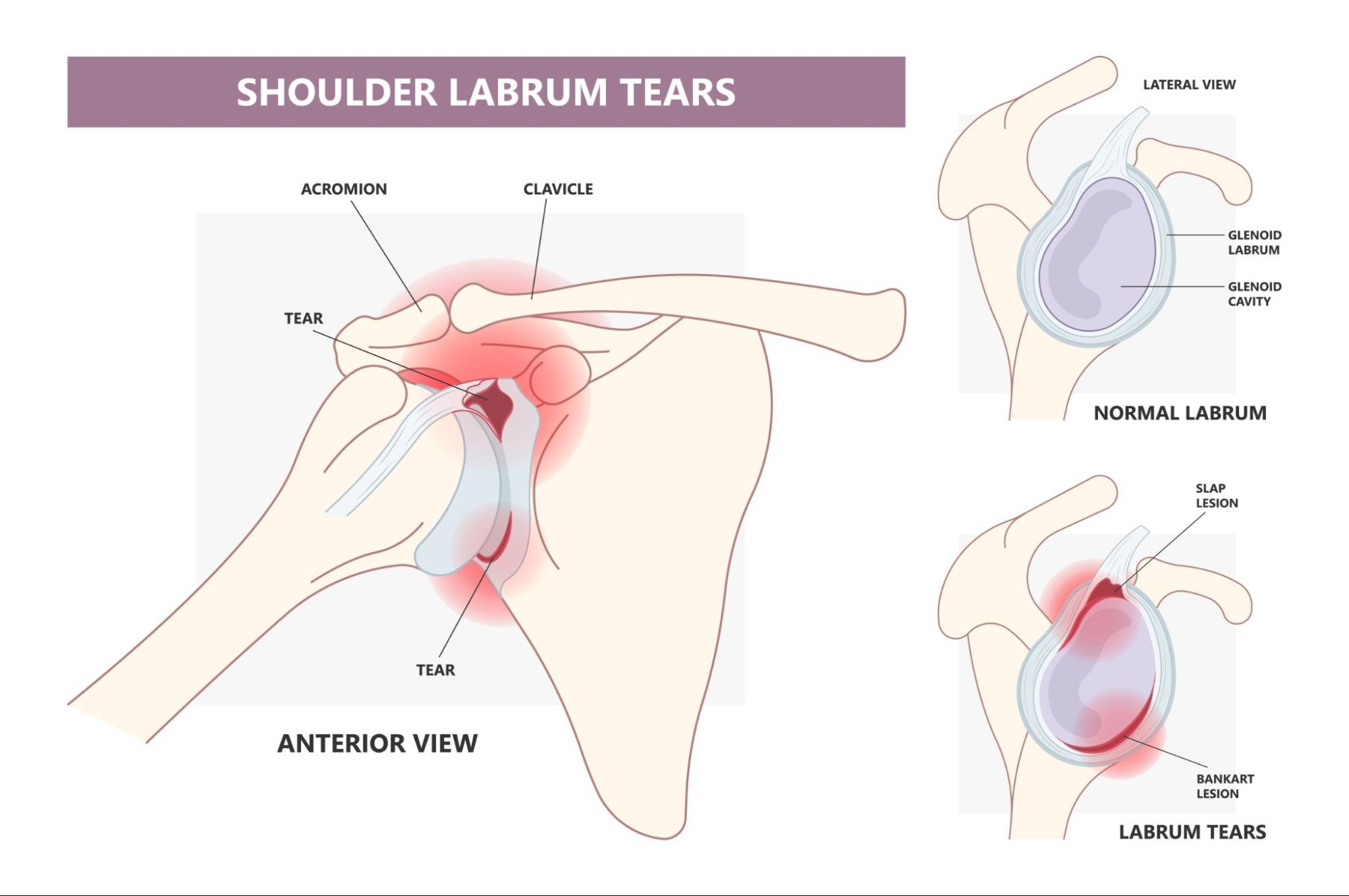
Another injury that can occur at the shoulder as result of playing tennis (or other sports) is something known as a SLAP lesion. This is an injury to the Superior Labrum Anterior-Posterior (SLAP) structure of the shoulder. In plain English, this translates as: the upper cartilage rim of the socket, extending from front to back.
Whilst these injury conditions can have unique characteristics, many share similarities in their symptom presentation because the structures that they affect are positioned closely together. Therefore, it is important to ensure that your shoulder pain is diagnosed correctly due to subtle differences in the way your recovery should be managed. More on that a little bit further down.
The Tennis Serve
Tennis is a physically demanding sport that involves repetitive actions and requires a great deal of strength, power and coordination to perform. If you are unaccustomed to these demands or if you rapidly increase your training load, you may be at increased risk of developing an injury.
One of the most physically demanding elements of tennis is the serve. The tennis serve is a high energy action that requires coordination of the kinetic chain throughout the body. It is also a common cause of tennis related shoulder pain.
The tennis serve can be broken down into five phases:
- The wind up
- Early cocking
- Late cocking
- Acceleration
- Follow through
Throughout these phases, the legs, hips, trunk, shoulder, elbow and wrist work through coordinated movements to produce the forces required for an effective serve.
On average, championship tennis players generate a ball speed of 170-180km/h (females) and 190-200km/h (males) when serving, which requires huge strength and power. It has been calculated that over 50% of the total force and kinetic energy of a serve is generated from the legs, hips and trunk.
If there is a breakdown in the kinetic chain from your legs or trunk, your serve can be compromised. To “catch up” and maintain an effective serve, compensations in movement patterns or force generation can occur. These typically happen at the shoulder and make it more susceptible to injury.
So, why is all this relevant? Well, over time, compensations due to inefficiencies elsewhere in the body can lead to movement dysfunctions or muscle imbalances at the shoulder.
In turn, these lead to shoulder pain caused by the repetitive compression or traction of shoulder structures, such as tendons bursae or labrum. Therefore, identifying it is important to identify the root cause of your symptoms. Treating local symptoms alone is unlikely to resolve your injury and result in your symptoms persisting or returning.
Symptoms
Common symptoms that you may experience at the shoulder as a result of these tennis related stresses include:
- Pain, particularly over the “badge patch” area of the upper arm
- Pain when you lift your arm
- Weakness of the shoulder muscles
- Increased pain at night – a sign of pain caused by inflammation of shoulder structures
- Clicking when you move the shoulder
- The feeling that your shoulder is loose or might slip out of place (more commonly associated to SLAP lesions)
Diagnosis
The physiotherapists at Complete Physio are highly trained specialists capable of diagnosing your shoulder pain because of playing tennis or taking part in other activities. Physiotherapists can diagnose your shoulder pain by undertaking a comprehensive clinical assessment that involves an interview and physical examination.
The interview seeks to understand the history, mechanism and pattern of your symptoms whilst the physical examination aims to localise the affected structures. This is achieved by assessing movement quality, strength and structural integrity of the affected area.

As identified, many shoulder problems can have similar clinical presentations, which can make it hard to accurately diagnose a shoulder injury from clinical assessment alone. This is where Diagnostic Musculoskeletal Ultrasound, a highly effective imaging tool to accurately detect shoulder pathologies can be used.
Many of the physiotherapists at Complete Physio are trained in and may use this to confirm your diagnosis.
Treatment
Most cases of shoulder pain can be resolved with conservative treatment, meaning there is no need for invasive procedures like surgery. Seeing a physiotherapist familiar with the demands and injuries of the sport is therefore essential. Failure to do so may result in ineffective rehabilitation and therefore a recurrence of symptoms.
Our team at Complete Physio understand these demands and can effectively rehabilitate you from injury. Your treatment is likely to include:
- Advice on activity modifications and ways to manage your symptoms
- Prescription of an effective rehabilitation programme to restore any imbalances or movement dysfunctions. This should include appropriate strength training and may include whole body exercises, not just focused on the shoulder. Afterall, it may be a weakness elsewhere in the body that has resulted in your shoulder taking the brunt of the stress and causing pain
- Appropriate progression of your rehabilitation exercises to ensure a safe return to play. This is essential as the exercises at the end of your rehabilitation should be somewhat different to those at the start. Your rehabilitation needs help you overcome your initial symptoms and ultimately prepare you to cope with the physical demands of the sport
- Application manual therapy techniques, such as soft tissue massage or joint mobilisations to alleviate symptoms and enable you to complete your exercise programme
- Shockwave therapy to stimulate a healing response
- Corrective taping techniques to alleviate pain and facilitate correct movement patterns at the shoulder
In some cases, it may be appropriate to consider an ultrasound guided injection to alleviate symptoms. Injection therapy has been used to treat musculoskeletal conditions for many years and can be highly effective in cases with particularly severe or persistent symptoms.
Current best evidence suggests that injection therapy as a standalone treatment is less effective than when used in combination with physiotherapy to treat musculoskeletal conditions. The advantage of Complete Physio is that there are physiotherapists who can do both for you and manage your injury throughout: from diagnosis to return to play.
Summary
If you are experiencing shoulder pain because of your tennis game, it is important to recognise that there can be several causes. The structures in your shoulder that become affected can vary, but often present with similar, often pain related symptoms. Among the causes are the biomechanics of how you move on-court, or how physically prepared you are to cope with the demands of the sport.
Although tennis-related shoulder pain is fairly common, most cases are not serious (i.e., not harmful to health) and can often be resolved with good quality physiotherapy. In cases where symptoms are deemed severe or persistent, an ultrasound guided injection may be required in addition to physiotherapy to achieve full symptom resolution.
For more information or to book an appointment
please call 020 7482 3875 or email info@complete-physio.co.uk
References
Daniels, E.W., Cole, D., Jacobs, B. and Phillips, S.F., 2018. Existing evidence on ultrasound-guided injections in sports medicine. Orthopaedic journal of sports medicine, 6(2), p.2325967118756576.
Funk, L., 2022. SLAP Lesions | ShoulderDoc. [online] Shoulderdoc.co.uk.
Lawn Tennis Association. 2022. Tennis in London. [online]
van der Hoeven, H. and Kibler, W., 2006. Shoulder injuries in tennis players. British Journal of Sports Medicine, 40(5), pp.435-440.