Spondylolisthesis
What Is Spondylolisthesis?
Spondylolisthesis is a spinal condition which involves translation of one the vertebrae (bones in your spine) relative to the adjacent vertebrae. It is not a very common condition; it only occurs in about 4-6% of the adult population. It can occur anywhere along the spine, but is most common in the lumbar region (low back). In the vast majority of cases symptoms can be managed conservatively with physiotherapy, however in more severe cases, especially if one of the spinal nerves or spinal cord is being compromised, surgery may be required.
Anatomy of the Spine
Vertebrae
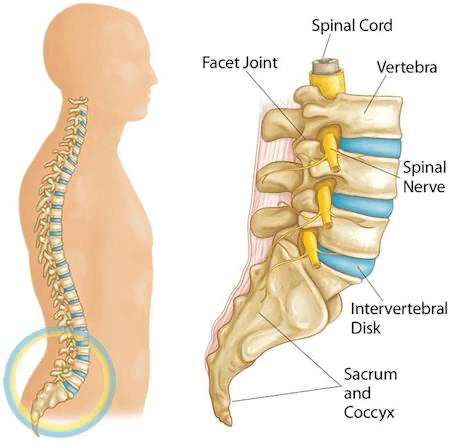
The spine is made up of small bones, called vertebrae, which are stacked on top of one another and create the vertebral column. This column creates a canal that houses and protects the spinal cord. It is also the structure that supports the body, and allows us to maintain an upright posture.
Facet Joints
Each vertebra has two facet joints, one each side, which join one vertebrae to another.
The facet joint surfaces are covered in a very smooth layer of cartilage which minimises joint friction.
These joints create a tripod complex with the intervertebral discs, which keeps the joint stable and strong, while at the same time allows movement.
Intervertebral Discs
The intervertebral discs are a cushion of fibrocartilage which sit between each vertebrae in the spinal column and act as shock absorbers when you move, jump, walk or run.
Spinal Nerves
The spinal nerves exit just above the facet joint at each level, and provide sensory and motor control to the body.
What Causes Spondylolisthesis?
There are two main causes of Spondylolisthesis:
- Spondylolysis
- Degeneration (‘wear and tear”) of the spine
1) Spondylolysis
Sometimes a stress fracture can develop in one of the vertebrae - a condition known as Spondylolisis. A stress fracture occurs due to repetitive high force on the lower back. This can occur with sports such as fast bowling and rugby. If this worsens and turns into a complete fracture (known as a “pars fracture” - see image below), the vertebra can slip forwards onto the vertebrae below resulting in Spondylolisthesis.
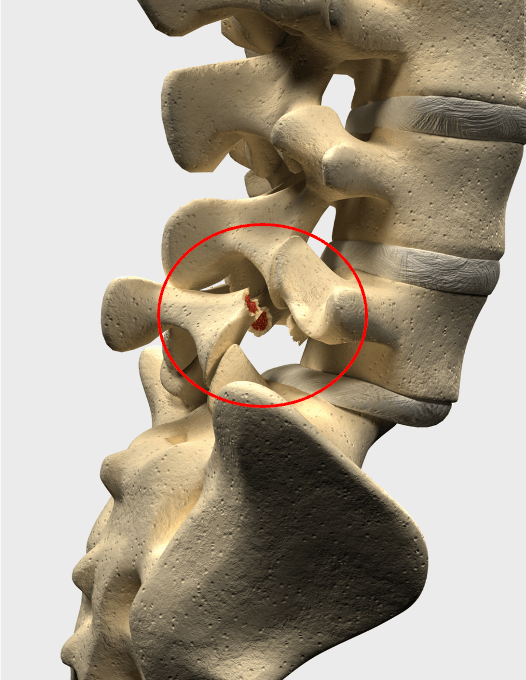
A “Pars fracture”
2) Degeneration of the Spine
As we age, our joint surfaces go through changes; the cartilage and discs between the vertebrae and the facet joints can wear down and become thin.
This is a normal ageing process and often goes unnoticed, but in some cases it can cause inflammation to the joints and bones. This inflammation triggers a natural healing response; as the body tries to repair itself it can overstimulate the growth of bone on the joint surfaces. These are referred to as ‘bony spurs’. These spurs cause an unstable and uneven surface area, which pushes the vertebrae out of place and is what leads to spondylolisthesis.
In addition to this, the ligaments along the back of the spine that help to hold the vertebrae together, also begin to weaken, potentially adding to the slippage.
On very rare occasions, as Spondylolisthesis develops, the spinal nerves and even the spinal cord can become compressed.
Other, less common causes include:
- Trauma - A high impact injury or trauma can cause a vertebra to slip out of place.
- Pathological - Another medical condition such as osteoporosis or a tumour can cause it.
- Congenital - It could be a defect in the vertebra from the time a person was born.
What are the symptoms of Spondylolisthesis?
As previously mentioned, Spondylolisthesis is most commonly seen in the lumbar spine but can also occur in the cervical or thoracic spine. Symptoms are experienced differently in every individual, and will depend on the spinal level affected. Some people don’t have any symptoms at all (asymptomatic). In most cases patients will likely experience intermittent back pain, which can extend into the buttocks and thighs (lumbar spine) or shoulders and arms (cervical spine).
Other common symptoms include:
- Muscle tightness and muscle spasms in the lower back or hamstrings
- Joint stiffness in the lower back or neck
- Tingling, numbness, or pins and needles in legs, feet, arms or hands
- Sciatica pain
- Swayback posture
- Increased symptoms when arching the back or extending the neck.
- Weakness in legs or arms
- Difficulty with standing or walking
- Pain that worsens with activity
At Complete Physio we are experts in the diagnosis and treatment of spinal pain. If you have any of the above symptoms, please contact us today to book an appointment.
IMPORTANT: You should be aware that if you are suffering from symptoms of extreme bilateral leg (both legs) weakness, numbness or severe pins and needles in the groin or genital area, or loss of bladder or bowel control/function, you should seek medical help immediately, as these can be symptoms of a more serious condition called cauda equina syndrome, which needs emergency treatment and you should attend A&E.
How is Spondylolisthesis Diagnosed?
It’s essential to get an accurate diagnosis of your problem to ensure that you are started on the best and most effective treatment plan. Our physiotherapists at Complete Physio are highly skilled diagnosticians; they will carry out a comprehensive assessment of your spine and will be able to give you a clear explanation of your diagnosis.
Medical History
At your initial appointment your Physiotherapist will firstly listen to your account of the problem and take a subjective history; asking you questions about your past health, symptoms, normal daily routine and activity level. They will ask more specific questions about the type and location of your pain and what other symptoms you are experiencing.
This will help to build up a picture of what is likely to be the cause of the problem.
Clinical Examination
After your subjective consultation, the specialist will complete a series of clinical tests to confirm their diagnosis; this may include:
- Observing you walking, bending, squatting.
- Testing spinal range of movement.
- Palpating the spine to assess the position and movement of the individual vertebrae and joints in the spine, and feeling the surrounding spinal muscles and soft tissue structures.
- Testing muscle strength of your lower legs or arm muscles
- Assessing sensory and motor impairment
- Testing your lower or upper limb reflexes
- Observing your spinal posture
- Looking at your pelvic and core stability.
Special Imaging Tests for Spondylolisthesis
It may be appropriate for you to have imaging tests to help confirm your diagnosis and identify the location and extent of a slipped vertebra, and whether there is damage to the surrounding bones or nerves. At Complete Physio our clinicians can refer you directly for imaging tests to ensure we get the correct diagnosis. We can also refer you to world leading spinal consultants and surgeons if we feel you require further input to ensure we optimise your treatment plan.
X-rays
In most cases an x-ray is sufficient to diagnose Spondylolisthesis. X-rays visualise bones and will show whether a lumbar vertebra has slipped out of place. They will also show degenerative bone and joint changes that occur with ageing, such as loss of joint space or bone spurs.
X-rays can also be used to grade the severity of your Spondylolisthesis; the grading scale below is based on how far forward a vertebral body has slid forward over the vertebra beneath.
- Grade I: Less than 25% slip
- Grade II: 25% to 49% slip
- Grade III: 50% to 74% slip
- Grade IV: 75% to 99% slip

MRI (Magnetic Resonance Imaging)
MRI scans create better images of soft tissues, such as muscles, discs, nerves, and the spinal cord than x-rays do. They can also show the slippage in more detail and whether any of the nerves are pinched.
Our physiotherapists are able to refer you for an MRI scan if required; you do not need a GP referral for this. Please contact our admin team on 0207 482 3875 or email info@complete-physio.co.uk if you know that you would like to see a physiotherapist and will also require an MRI scan.
Computed Tomography (CT)
CT scans create cross-section images of your spine, and show bony detail better than MRI, however MRI is superior when analysing nerve involvement/injury.
How do we Treat Spondylolisthesis?
Physiotherapy
Non-surgical treatment should always be the first line of intervention. Physiotherapy treatment for spondylolisthesis will generally focus on reducing pain and muscle spasms, improving spinal stability and restoring function. Your physiotherapist will use a variety of techniques, including hands on soft tissue treatment, posture and movement reeducation, and targeted exercises to help you to settle your symptoms and regain normal movement and function.

At Complete we believe in a patient centred, holistic approach, therefore treatment programmes vary, depending on what your therapist finds during your clinical assessment. They will tailor your programme to specifically help you and your individual needs and goals.
Treatment may include:
- Rest and advice on avoiding certain activities or movements. In more severe cases, some patients may need to wear a back brace for a period of time to limit movement in the spine and allow a recent pars fracture the opportunity to heal.
- Pain medication such as paracetamol and/or anti-inflammatory medicines like ibuprofen or naproxen, are often useful. If the nerve is being irritated then drugs such as amitriptyline or gabapentin may be prescribed. This should always be discussed with a pharmacist or GP who can prescribe the most appropriate pain relief for you.
- Exercises are targeted on engaging the deep spinal stabilising muscles in your back and abdominals, as well as improving your movement patterns and posture.
- As your symptoms improve, your physiotherapy programme will likely progress to work on improving your flexibility, strength and function, and on helping you to return to your normal exercises and activities.
- Your physiotherapist may also suggest that you commence a course of Pilates and rehabilitation, which is a highly effective way of managing mechanical low back pain.
- Manual therapy e.g. joint manipulation and/or mobilisation, as well as soft tissue techniques targeted to the surrounding joints and soft tissues can provide rapid pain relief and improve full range of movement of the spine.
- Acupuncture has been shown to be an effective treatment option for back and neck pain. Acupuncture has been proven to help with muscle spasm, improve blood circulation, regulate the nervous system, and release neurotransmitters to reduce pain. Many of our physiotherapists utilise acupuncture or dry needling as part of their treatment.
The length of recovery may vary, but a comprehensive rehab programme typically takes several weeks to a few months of supervised physiotherapy treatment. Your Physiotherapist will ensure that you feel supported throughout your treatment programme, and they will continually reassess your symptoms and progress to make sure that you reach your goals.
What are my options if Physiotherapy is not helping?
Spinal Injections for Spondylolisthesis
Spinal injections are a common, relatively low risk way of treating pain from spondylolisthesis. If your symptoms are not settling with physiotherapy alone, or if your pain is so severe that you are not able to engage in your rehabilitation programme, then spinal injections might be an option for you.
Spinal injections involve a mixture of local anaesthetic and corticosteroid (a potent anti-inflammatory) being injected into the lower back. This can be very effective in reducing the discomfort, swelling and inflammation in the spinal joints, surrounding soft tissue and injured nerve roots.
The purpose of the injections is to reduce pain to a level that enables the patient to completely engage in and benefit from a physiotherapy programme and should never be a stand alone treatment.
If your Physiotherapist feels that this treatment is required, they will be able to refer you to one of the highly experienced and well trusted Spinal Consultants that we work closely with. These injections are not carried out at Complete Physio.
Surgery
Although non-surgical treatment is often very successful, sometimes surgery is required to relieve the symptoms of spondylolisthesis and prevent the condition from worsening.
The type of surgery performed for spondylolisthesis varies depending on the symptoms that are being caused and the amount of vertebral slippage.
Spinal Decompression
This is a relatively small and straightforward operation to relieve pressure on a nerve root. There are a number of techniques that can be used, and the exact operation will be decided with your specialist. It can sometimes be used as a stand alone operation, however, it is more commonly used in combination with a spinal fusion.
Spinal Fusion
This is the most common procedure used for spondylolisthesis. Spinal fusion stabilises the spine by permanently joining two vertebrae, eliminating movement between them. Typically, bone grafts are placed between vertebrae to help them fuse together. In time, new bone grows over the graft. A surgeon will also place small metal screws and rods into the spine to hold the vertebrae together while they heal and fuse. This is a bigger and more complex operation to realign your spine and is used when you have a severe spondylolisthesis.
We work with some of the most experienced and specialist spinal surgeons in the country, so if an onward referral to a surgeon is needed, we will ensure that you are provided with the best care possible. Following surgery we will continue to support your post op recovery and rehabilitation every step of the way.
We have a number of Complete Physio clinics across London, and can usually offer next day appointments. If you would like to book an appointment or speak to one of our expert physiotherapists about your condition, please call 020 7482 3875 or email info@complete-physio.co.uk.