Achilles Rupture – Surgery vs Conservative Treatment
An Achilles tendon rupture can heal without surgery using a modern functional rehabilitation protocol, and outcomes are comparable to surgical repair for most patients.
A well regarded randomised controlled trial, published in the New England Journal of Medicine 2022, found no significant difference in patient-reported outcomes between surgery and conservative treatment at two years.
Recovery without surgery follows a structured boot and loading programme spanning 9-12+ months to return to running and sport. This can be longer if your sport involves sprinting and cutting movements.
When a patient comes into one of our central London clinics having just ruptured their Achilles, often after feeling a "pop" during a sprint or jump, the first question is almost always - ‘do I need surgery?’
Twenty years ago, the answer for any active adult was almost certainly yes. Today, the evidence has shifted considerably.
At Complete Physio, we've guided hundreds of patients through conservative Achilles rupture recovery, and the outcomes, when the protocol is followed correctly, are excellent.
Here's what that actually looks like.
Key Takeaways
- Surgery is not always necessary: The 2022 trial demonstrated comparable 2-year outcomes between surgical and conservative management for complete Achilles rupture, challenging the previous default towards operative repair
- Modern conservative treatment is functional, not passive: Current protocols involve controlled early weight-bearing in a boot - not six weeks in a plaster cast - which produces significantly better tendon healing
- Early Assessment is absolutely vital: In order for conservative management to be successful, you need to get a diagnosis and have your ankle immobilised within 48hrs.
- Re-rupture risk with modern protocols is low: Well-managed functional rehabilitation carries a re-rupture rate of approximately 3 - 4%, comparable to surgical rates of 2 - 3%
- Patient selection matters: Age, activity level, rupture gap, and time since injury all influence whether conservative or surgical management is the better choice
- Return to running and sport takes 9 - 12 months: Regardless of treatment route. Return to high-level sport involving sprinting and cutting typically takes 12+ months
What Is an Achilles Tendon Rupture and How Does It Happen
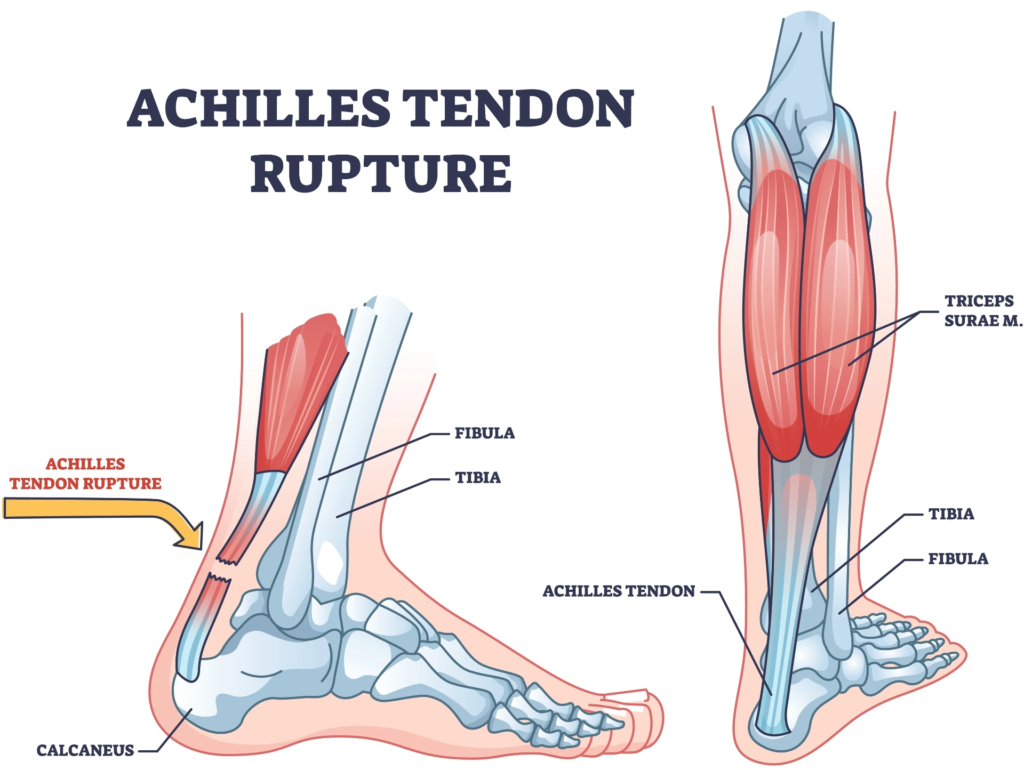
An Achilles tendon rupture is a complete or partial tear of the tendon connecting the calf muscles to the heel bone, usually occurring 2-6 cm above the heel, during a sudden, forceful push-off or change of direction.
The Achilles tendon is the largest and strongest tendon in the body, capable of withstanding forces of six to eight times body weight during running.
Despite this, it remains one of the most commonly ruptured tendons; primarily because it has a relatively poor blood supply in the mid-portion, making it vulnerable to degenerative change over time.
The classic mechanism is a sudden, explosive movement: a sprint start, a jump landing, a rapid change of direction in racket sports.
The injury is most common in men aged 30 - 50 who are recreationally active - the so-called "weekend warrior" demographic - though it also occurs in elite athletes and older, less active individuals.
Risk factors that increase Achilles rupture likelihood include:
- Previous Achilles tendinopathy or a history of tendon pain
- Use of corticosteroid injections near the tendon
- Sudden return to sport after a period of inactivity
- Being male (rupture is 4-5 times more common in men)
- Excess body weight increasing load per stride
Diagnosis of Achilles Rupture
Diagnosis can usually be done with a straightforward clinical assessment.
If the tendon is ruptured, the ‘Thompson test’ - which involves squeezing the calf with the patient lying on their front - produces no foot movement. In a normal tendon this test causes the foot and toes to point. Additionally, there is often (but not always) a palpable gap/defect at the mid portion of the tendon.
Ultrasound-guided decision making
Diagnostic Ultrasound is often used to confirm the diagnosis and helps determine rupture gap size. This information is really useful when deciding between conservative and surgical management.
One of the defining features of treatment was the use of dynamic ultrasound.
Patients are scanned with the ankle in plantarflexion to assess:
- Tendon gap size
- Tendon end apposition
- Continuity during positioning
At complete physio, we have clinicians trained in musculoskeletal sonography, who are able to carry out a diagnostic ultrasound in clinic at the same time as your initial assessment.
If you think you might have this injury, it is best to ensure you are booked in with one of our clinical specialists who can perform this imaging assessment. Make sure you make this clear at the time of booking your appointment.
What Does Conservative Treatment for Achilles Rupture Involve?
There are a number of studies and protocols for conservative management that treatment is based on.
The Swansea Morriston Achilles Rupture Treatment (SMART) programme is a physiotherapy-led accelerated functional rehabilitation pathway for Achilles tendon rupture developed at Morriston Hospital and introduced in 2008.
It aims to reduce unnecessary surgery while maintaining low re-rupture rates through early functional rehabilitation and ultrasound-guided decision making.
Core principles of the programme
The pathway includes:
- Early specialist ultrasound assessment
- Functional bracing instead of prolonged casting
- Early weight bearing
- Accelerated rehabilitation
- Physiotherapy-led progression
- Ultrasound-based selection for surgery vs conservative care
- Structured return-to-work and return-to-sport guidance
Conservative treatment for Achilles rupture means functional rehabilitation in a removable boot with progressive weight-bearing - not plaster casting or prolonged rest.
This distinction is really important.
The older approach to non-surgical management involved many weeks of non-weight-bearing plaster cast immobilisation, which produced poor outcomes and high re-rupture rates.
That's the version that earned conservative treatment its historical bad reputation. Modern functional protocols are fundamentally different.
The conservative protocol typically follows this structure:
- Days 0-14: Removable walking boot fitted with heel wedges to bring the foot into plantarflexion (toes pointing down), partially approximating the ruptured tendon ends. Partial to full weight-bearing as tolerated with crutches for comfort
- Weeks 2-6: Gradual removal of heel wedges (one wedge every 1–2 weeks), progressive full weight-bearing. Daily non-resisted range-of-motion ankle exercises.
- Weeks 6-12: Transition out of the boot into normal footwear, introduction of bilateral and then unilateral calf raises, neuromuscular training, walking gait retraining
- Months 3-6: Progressive tendon loading programme (slow, heavy calf raises), jogging preparation, proprioception and balance training
- Months 6-14: Return-to-sport programme: straight-line running → change of direction → sport-specific drills → full return
Physiotherapy is not optional in this process, it drives every phase of it.
Without structured guidance, patients either under-load the tendon (risking elongation and persistent weakness) or overload it (risking re-rupture).
The protocol is the treatment!
Is Conservative Treatment as Effective as Surgery for Achilles Rupture?
For most patients, conservative, functional rehabilitation produces outcomes equivalent to surgery at two years, with lower complication rates and no surgical risks.
The strongest evidence comes from a trial published in the New England Journal of Medicine in 2022.
This multicentre randomised controlled trial recruited 526 patients with complete Achilles rupture across 39 UK hospitals. At two years, there was no statistically significant difference between surgical and non-surgical groups on the primary outcome measure (Achilles Tendon Rupture Score), functional testing, re-rupture rates, or return to activity levels.
Key findings from the 2022 trial and supporting literature:
- Re-rupture rates: Conservative 3.5% vs surgical 2.3% - a small absolute difference that is not statistically significant
- Complication rates: Surgical patients had higher rates of wound infection, nerve damage, and deep vein thrombosis than conservatively managed patients
- Return to sport: No significant difference in return-to-sport rates between groups at 2 years
- Tendon elongation: This remains more common after conservative treatment and is a genuine concern - requiring careful monitoring and targeted loading to address
Surgery retains advantages in specific patient groups, particularly elite athletes for whom even a small reduction in re-rupture risk or a marginal improvement in tendon stiffness justifies operative intervention.
But the blanket assumption that surgery is always superior is no longer supported by the evidence.
Who Is a Good Candidate for Conservative Achilles Rupture Treatment?
Conservative treatment is appropriate for most adults with a complete Achilles rupture who present promptly and have a small-to-moderate rupture gap - typically under 5mm on ultrasound in plantarflexion.
At Complete Physio, our assessment process for Achilles rupture includes clinical examination, Thompson test, and urgent ultrasound imaging to measure the rupture gap in plantarflexion (the position the foot will be held in the boot).
This gap measurement is the single most important factor in patient selection for conservative management.
Conservative management is generally preferred when:
- The rupture gap is small or the tendon ends are in close proximity in plantarflexion
- The patient presents within 48 - 72 hours of injury (earlier intervention allows the tendon ends to be held in optimal position)
- The patient has significant medical comorbidities that increase surgical risk (diabetes, peripheral vascular disease, obesity)
- The patient is over 60 and moderately active (lower functional demands)
- The patient's occupation or personal circumstances make post-surgical immobilisation impractical
Surgery may be preferred when:
- The rupture gap is large (>5mm in plantarflexion) - the tendon ends cannot approximate sufficiently for conservative healing
- The patient presents in clinic late (more than 4 weeks after injury) and retraction has occurred
- The patient is a competitive athlete for whom maximum tendon stiffness and the lowest possible re-rupture risk are priorities
- There has been a previous Achilles rupture on the same side
The decision should always be made jointly between the patient, their physiotherapist, and an orthopaedic surgeon, and after imaging, not before.
What Is the Week-by-Week Recovery Timeline Without Surgery?
Conservative Achilles rupture recovery follows a 9 - 12 month timeline, with distinct phases progressing from protected weight-bearing through to full return to sport.
The timeline below reflects typical progression. Individual variation is significant; age, body weight, fitness level, and adherence to the programme all affect speed of recovery.
Rushing any phase increases re-rupture risk.
Non-operative rehabilitation protocol
Phase 1: Protection (Weeks 0 - 2)
Immobilisation
- Below-knee cast (this is often put on if you attend A&E) or boot in maximal equinus/plantarflexion
- Tendon ends approximated in dorsiflexion (foot and toes down) immediately after diagnosis
- Should be applied within 24 - 48 hours
- If in a boot it needs to be worn day and night
Weight bearing
- Early protected/partial weight bearing with crutches encouraged
Exercises
- Toe movement
- Knee ROM
- Hip strengthening
- Cardiovascular conditioning where safe
Primary goal: prevent further tendon separation and begin early soft tissue healing.
No active foot movement at this stage.
Phase 2: Controlled Loading and Early Functional Rehab (Weeks 2 - 6)
Transition to VACOped-style boot
At approximately 2 weeks:
- If you’re in a backslab/cast, this is removed
- Functional boot fitted with heel wedges
- Ankle maintained in plantarflexion
Weight bearing (WB)
- Progression toward full weight bearing
- Typically:
- week 2-3: partial WB
- week 4-6 onward: WBAT/full WB in boot
ROM
Allowed from approx 4 weeks :
- Daily active plantarflexion
- Gentle ankle movement toward neutral
Avoid:
- Dorsiflexion beyond neutral
- Any calf stretching
Exercises
- Seated calf activation
- Proprioception work in boot
- Stationary bike with protection
- Full weight-bearing by week 6.
- First physio assessment of calf activation.
Boot progression
- Progressive removal of heel wedges from 6 weeks.
- Ankle brought progressively toward neutral
The emphasis is on controlled tendon loading rather than immobilisation.
Phase 3: Rehabilitation Progression (Weeks 6 - 12)
Boot Transition
- Gradual move from boot to normal footwear
- Heel raise often used initially in shoes
Rehabilitation
- Bilateral calf raises begin (both legs together), progressing to single-leg as strength allows.
- Theraband strengthening
- Balance training
- Closed-chain strengthening
- Pool work if available
Goal: achieve 20 single-leg calf raises before progressing further. Running and jumping should still be avoided at this stage.
Phase 4: Progressive Tendon Loading (Months 3 - 6)
- Heavy slow resistance calf programme - the same protocol used for Achilles tendinopathy.
- Balance and proprioception training.
- Light jogging preparation on a static bike, pool running, or AlterG (anti gravity) treadmill.
Phase 5: Return to Running (Months 6 - 9)
- Graduated return-to-run programme (walk-jog intervals, progressing to continuous running).
- Plyometrics
- Hopping and landing mechanics
Strength criteria: single-leg calf raises ≥90% symmetry, passing limb symmetry index on hop tests.
Phase 6: Return to Sport (Months 9 - 12+)
- Sport-specific training, change of direction, reactive drills.
- Clearance based on objective testing, not timeframes.
- Athletes returning to high-demand sport should not rush this phase.
What Are the Risks of Conservative Achilles Rupture Treatment?
The primary risks of conservative Achilles rupture treatment are re-rupture (3 - 4%), tendon elongation with residual weakness, and the requirement for consistent patient commitment over a 9-12 month rehabilitation period.
Re-rupture is the risk patients worry about most. With a properly supervised functional protocol and good boot compliance, the absolute risk is low, and comparable to the 2–3% re-rupture rate seen after surgery.
Most re-ruptures occur when patients remove the boot too early, try to push through pain in early phases, or skip physiotherapy.
Tendon elongation is a subtler but clinically meaningful risk.
When the Achilles heals in a lengthened position - which is more common without surgery - the calf muscle loses mechanical advantage.
This manifests as persistent weakness during single-leg calf raises and reduced push-off power during running. Addressing tendon elongation requires specific heavy loading over many months and, in some cases, is never fully resolved.
Conservative treatment also demands significantly more from the patient than surgery does. Post-surgical patients have a clear wound-healing period that enforces relative rest.
Conservative patients must actively manage their loading throughout; attending physiotherapy, progressing exercises correctly, and resisting the temptation to return to activity too soon.
Poorly adherent patients consistently have worse outcomes regardless of treatment route.
What Does Physiotherapy Involve During Conservative Achilles Rupture Recovery?
Physiotherapy drives every phase of conservative Achilles rupture recovery - from initial boot fitting and load management through to functional testing and return-to-sport clearance.
In the early stages, we assess rupture gap on ultrasound (or liaise with radiologists who have), confirm boot positioning, prescribe appropriate heel wedge height, and establish safe weight-bearing parameters.
We also begin the work of managing the patient's anxiety and expectations - recovery without surgery is a long road and patients need to understand each phase before it begins.
Through the strengthening and loading phases, physiotherapy involves:
- Progressive loading prescription: calculating the right resistance, tempo, and volume for each week of the programme
- Gait analysis: identifying compensatory movement patterns that develop during boot wearing and correcting them before they become entrenched
- Tendon monitoring: tracking tendon structure on ultrasound where available, and monitoring elongation
- Neuromuscular training: restoring balance, proprioception, and reactive control that are lost during the injury and boot period
- Return-to-run testing: objective limb symmetry assessments (hop tests, calf raise endurance, isometric strength testing) before any running is introduced
At Complete Physio, we use a combination of hands-on treatment, exercise prescription, and - where appropriate - adjuncts such as shockwave therapy for cases complicated by tendinopathy in the healing tendon.
Our physiotherapists have direct experience managing both surgical and non-surgical Achilles ruptures and will work with your surgeon if operative management is being considered or has already occurred.
Frequently Asked Questions
How do I know if I've completely ruptured my Achilles or just strained it?
A complete rupture typically causes a sudden, severe pain, often described as feeling like you were kicked from behind, followed by a distinct pop or crack.
You'll be unable to stand on your tiptoes on the affected leg.
The Thompson test (calf squeeze with you lying face down) will show no foot movement on the injured side. A partial tear or strain produces localised pain without these functional deficits. If you're unsure, urgent physiotherapy or A&E assessment with ultrasound is the correct next step - don't wait!
Can I walk if I've ruptured my Achilles?
Many patients can walk after a complete Achilles rupture - often with a limp and significant pain.
The ability to walk does not rule out a complete rupture, as other muscles (flexor hallucis longus, peroneal muscles) partially compensate.
Walking on an undiagnosed rupture before fitting a boot increases the risk of the tendon ends separating further, which makes conservative treatment harder and surgery more likely.
Seek assessment the same day if possible.
What does the boot feel like and how long will I need to wear it?
The boot is a removable walking cast that holds your foot in a toes-down position (plantarflexion), keeping the tendon ends close together while healing begins.
There are different types of boots that are used, but we recommend the vacoped boot.
Most patients wear it full-time (removing only for showering with the foot in the correct position) for 8 - 10 weeks, progressing from full plantarflexion to neutral over that period. Initially it feels awkward and slightly unsteady - an even-up shoe for the other foot helps normalise your gait and reduce back strain.
Will my Achilles ever be the same after a rupture?
Most patients return to their pre-injury activity levels - running, sport, and normal life - after a complete Achilles rupture, whether managed conservatively or surgically.
Research shows the majority of patients achieve this by 12 - 18 months. Some residual calf weakness or loss of explosive power is possible, particularly if tendon elongation has occurred. Elite athletes sometimes notice a performance ceiling in the year following injury.
With a complete, well-structured rehabilitation programme, significant functional recovery is the norm, not the exception.
Can I go to the gym during Achilles rupture recovery?
Yes, with guidance.
Upper body training, seated resistance machines (avoiding those requiring plantarflexion in the early weeks whilst in a boot), swimming (kicking optional later in recovery), and cycling on a stationary bike (once out of the boot) are all viable options at various stages.
Pool running with a flotation vest (to reduce weightbearing) maintains cardiovascular fitness without tendon loading. Your physiotherapist will give you specific clearance for each activity based on your current phase of healing.
Is shockwave therapy useful for Achilles rupture recovery?
Shockwave therapy is not a first-line treatment for acute Achilles rupture, it's most relevant during later phases of recovery if the healing tendon develops areas of tendinopathy (degeneration) or calcification.
Some clinics use low-energy shockwave early in recovery to stimulate collagen production, but this is not yet standard practice.
Shockwave has stronger evidence for chronic Achilles tendinopathy that hasn't responded to loading exercises.
Does the conservative protocol work for older patients?
Yes, conservative treatment is often the preferred approach for patients over 60.
Older patients typically have lower functional demands, higher surgical risk, and equivalent patient-reported outcomes with non-operative management. The same functional protocol applies, though recovery timelines may be modestly longer.
Age alone is not a barrier to full recovery from Achilles rupture - we regularly treat patients in their 60s and 70s back to full activity.
What happens if I choose conservative treatment but it fails?
If the Achilles tendon fails to heal adequately with conservative management, either due to re-rupture, excessive tendon elongation, or persistent functional deficit, surgical reconstruction remains an option.
Late (chronic) surgical repair is technically more challenging than primary repair and outcomes are generally less predictable, so it's a decision made carefully.
In practice, the majority of patients who follow the conservative protocol correctly do not require subsequent surgery.
How do I know when I'm ready to return to sport?
Return-to-sport clearance is based on objective testing, not time alone.
Standard criteria include: single-leg calf raise ≥90% repetition symmetry compared to the uninjured side, passing a battery of hop tests (single hop, triple hop, crossover hop for distance), and completion of sport-specific load exposure without pain or swelling.
Athletes who rush return to sport before meeting these criteria have consistently worse re-injury rates.
Getting Achilles Rupture Recovery Right
A complete Achilles tendon rupture is a serious injury, but it's not a career-ending one, and surgery is not always the answer.
The evidence is clear; a well-designed conservative protocol, delivered and supervised by experienced physiotherapists, produces comparable outcomes to operative repair for the majority of patients.
The key is starting it promptly, following it precisely, and resisting the urge to shortcut any phase.
If you've ruptured your Achilles or are unsure whether you have, get assessed quickly. The window for optimal conservative management is short - early diagnosis and treatment leads to better tendon approximation, better healing, and a smoother recovery.
Don't wait for the swelling to go down before seeking help.
About Complete Physio
Complete Physio is London's leading physiotherapy and sports injury clinic, with locations across London.
Our team of specialist physiotherapists are experienced in managing Achilles tendon injuries at every stage - from initial rupture assessment through to return-to-sport clearance.
References
- Myhrvold, S.B., Brouwer, E.F., Andresen, T.K., Rydevik, K., Amundsen, M., Grün, W., Butt, F., Valberg, M., Ulstein, S. and Hoelsbrekken, S.E., 2022. Nonoperative or Surgical Treatment of Acute Achilles’ Tendon Rupture. N Engl J Med, 386, pp.1409-20.
- Hutchison, A.M., Topliss, C., Beard, D., Evans, R.M. and Williams, P., The treatment of a rupture of the Achilles tendon using a dedicated management programme.
- Manent, A., López, L., Coromina, H., Santamaría, A., Domínguez, A., Llorens, N., Sales, M. and Videla, S., 2019. Acute Achilles Tendon Ruptures: Efficacy of Conservative and Surgical (Percutaneous, Open) Treatment—A Randomized, Controlled, Clinical Trial. The Journal of Foot & Ankle Surgery, 58(1229), pp.1229-1234
- Ochen, Y., Beks, R.B., van Heijl, M., Hietbrink, F., Leenen, L.P., van der Velde, D., Heng, M., van der Meijden, O., Groenwold, R.H. and Houwert, R.M., 2019. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. bmj, 364(k5120), p.1.