


At Complete Physio we treat many clients who have had a knee operation, be it an ACL reconstruction, an arthroscopy for a meniscal repair or a collateral ligament injury. One of the key questions we get from our clients following a knee operation is “when can I return to running/sport?

Whether your goal is to run a marathon or return to football we want to get you get back stronger and faster than before in the shortest possible time.
The principles of physiotherapy following these operations are very similar.
The key is not to rush the process and ensure you go back when you are ready. You will get different opinions about when you should return to running. It does depend on the knee operation but we always consider rehabilitation milestones rather than time frames. It’s only when you meet the milestones can you return to running/sport. This will ensure an optimal and safe return and avoid disappointment from returning too early. More importantly we must consider the long term health of your knee. Your knee has to survive for many years after an operation and incomplete or rushed rehabilitation is only to the long term detriment of your knee health.
How long it takes to return to running is also dependent on how strong the knee is before the operation. If you have had the knee problem for many years before the operation, it is likely that there is a reduction in the range of movement of the knee and significant muscle weakness. This is why we advise that you have pre-habilitation (rehab before your operation) if at all possible to get ready for the operation to ensure that you are as strong as possible beforehand.

There are five main areas we assess before we advise a client to return to running. Ideally you have achieved all 5 before returning to running/sport.
1. Knee swelling and range of movement
The knee should not be swollen and you should have achieved full range of movement. This obviously depends of the range of movement you had pre-operatively.
Self tests:
a) Do you have a swollen knee?
Swelling of the knee is not uncommon after a knee operation. By week 4 we would expect most of the swelling to have reduced. Any residual swelling normally accumulates around the top of the kneecap and/or just inside and outside of the kneecap.
We also do not want the knee to be swollen and certainly we do not want it to react to your rehabilitation exercises by swelling up after you have carried them out. If this is the case, then you are likely to still have a bit of reactive synovitis (inflammation of the joint lining) which is not uncommon following an operation but is something that needs to be monitored. It is unlikely that we would begin impact exercises if this is still the case such as hopping, jumping and running.
b) Do you have full flexion/bend of the knee?
Heel to bum and squat test
Full knee flexion generally means you are able to get your heel close to your buttock or at least as far the other side (if your other side is normal). You can also test your knee flexion by going into a full squat position with your heels off the ground and see if you can touch your heel onto your buttock with minimal pain or restriction.
c) Do you have full extension/straightening of the knee?
Squash your hand test!
By this we mean full extension or hyper-extension – depending on what your normal range of movement is on the other side.
Put your hand under your knee with the back of your hand touching the back of the knee crease. Push your knee straight by contracting your quadriceps muscle and feel how much pressure you have on your hand – try pulling your hand out and see how much resistance there is to moving your hand.
Essentially we would be looking for the same range of movement on both knees. Having symmetry is a good start.
2. Full strength of the knee
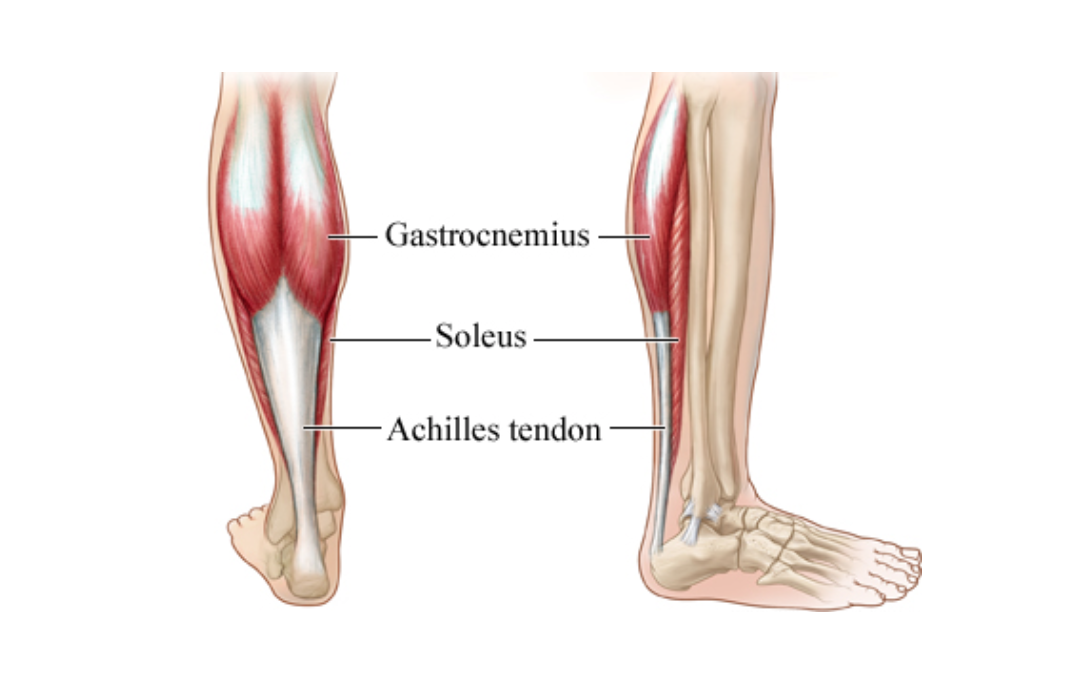
We would expect you to achieve all your strength goals before you start running. Running involves a lot of impact and the muscles are very important for absorbing force. For example, the soleus muscle (the main calf muscle) absorbs up to seven times your body weight whilst running.
It is very important that not only have you strengthened the muscles immediately above and below the knee such as the quadriceps, hamstring and calf complex but also that you have improved the strength of your foot musculature, and the muscles around the hip and core. Achieving excellent strength throughout the whole kinetic change will mean you are more likely to have a positive return to running. These muscles are absolutely key in ensuring you do not put too much load through the knee joint and will help to look after the long term health of your joint.
At Complete Physio, we use manual muscle testing using a hand held dynamometer and we also have an isokinetic machine which is the gold standard for measuring strength. Both of these provide objective data about your strength. This is what professional athletes use to know when they have achieved their strength goals and help decide when they should return to sport. We are one of the only clinics in London currently utilising isokinetic testing in clinic. It gives invaluable information, in terms of the strength difference from one side to the other and helps us to make the decision on return to running/sport. We expect there to be no more than 10% difference from the injured limb to the uninjured limb.

Handheld dynamometer
Isokinetic test
Your physiotherapist will assess your strength using specific tests and will prescribe you the correct exercises to ensure you get back to running/sport ASAP.
Self strength test:
To give you an idea of what strength you should be able to achieve before you return to running – try these tests:
1. You should be able to carry out 30 single leg (one leg) heels raises off a step taking 2 secs to lift up and 2 secs to drop down – so you must not bounce when you do the exercise and you must do it slowly not fast. That’s cheating! (See video below)
2. If you use a leg press you should be able to push one times your body weight for 10 repetitions. For example if you weigh 75kg you should be able to push 75kg on a leg press ten times. If you can’t you need to get stronger! For elite athletes or more experienced runners this should be 1.5 times your body weight. This may seem like a lot of weight but it is still less than the forces going through your knee when you run!
Research Corner: Why the leg press?
The purpose of this test is to assess the gluteus maximus (buttock) and quadriceps (front of knee), both very important muscles. Individuals with high levels of leg-press strength demonstrate high levels of knee dynamic joint stability and enhanced athletic performance. Clinical research demonstrates that knee injured individuals with high levels of leg press strength have better short and long-term recovery from knee injury and surgery. Low levels of leg press strength can, consequently, result in your achieving a lower level of knee dynamic joint stability, decrease your recovery from your knee injury or surgery, and increase your risk of re-injury
3. You should be able to carry out 30 single leg (one leg) hamstring bridges taking 2 secs to lift up and 2 secs to drop down – you must not bounce when you do the exercise and you must do it slowly, not fast. That’s cheating! (see video below)
3. Proprioception, balance and motor control.
Essentially this is the ability of the body to carry out certain activities with good balance, coordination and stability such as a single knee bend/squat. We will also look at your balance and your ability to change and correct position. This can be done through functional testing such as standing on one leg with your eyes open and eyes closed. We will also use things like a single leg squat and a small knee bend to assess your stability and compare to the other side.
Self tests:
1. Stand on one leg – you should be able to hold for 15 seconds without falling over or losing your balance! Start with your eyes open and then eyes closed. Research reports that individuals with impaired balance experience a higher number of lower limb re-injuries and new injuries than individuals with normal balance.
2. Stand on one leg and squat to approximately 70 degrees knee bend in front of a mirror. Ideally the front of your hip should be in-line with the middle of the knee and this should be in-line with the second toe (imagine a plumb line from the middle of your knee to your second toe – see first image below).
It is not uncommon that clients demonstrate poor alignment after a knee operation (see second image below). The most common compensation is where the knee moves medially i.e. the plumb line falls on the floor on the inside of the foot. If this is the case it is key to strengthen the lateral hip muscles particularly, but it also a sign of overall lower limb weakness or poor foot mechanics. Your physiotherapist will be able to devise a bespoke rehabilitation programme to correct these weaknesses before you return to running.
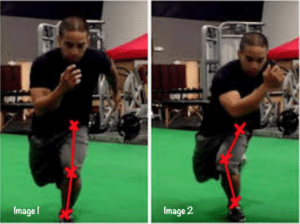
Single leg squat test
4. Functional performance tests (FPT’s)
These have been extensively researched, particularly following an ACL reconstruction and we generally use three tests. These have been used a battery of tests to help make the decision as to when to return to running. We often use the hop for distance, the crossover hop and the three hops for distance. Your physiotherapist will be able to carry these out with you in your session. These are excellent tests to highlight if there is any significant difference between the two limbs.
5. Confidence
Even when you have good strength and good balance, good range of movement and the knee is not swelling up, one of the key factors that determines re-injury rates is your own confidence in your knee. This is something that is difficult to measure but we do know that people are less likely to get re-injured and have a successful return to running/sport if they feel confident in their knee. If you don’t feel confident, then normally it is one of the components above that needs to be addressed. If you pass all our tests you are likely to feel very confident in your knee and get back to action!
We see many patients in our clinic who have returned to running too early and have not fulfilled the criteria above. It is important that all of the criteria are fulfilled before you can return to running. This article touches the surface of what we look at and we would always suggest that you come in for a full assessment to get a bespoke return to running/sport program specific for your needs and goals.
All our physiotherapists have extensive experience of working with patients who have had knee operations from Premier League footballers, Olympic to recreational athletes to the sedentary. We work with many of the leading knee consultants in London who refer directly to our clinic as we have formed an excellent relationship amongst our surgical colleagues for providing a comprehensive approach to rehabilitation.
If you have any questions or would like to speak to a physiotherapist to see if we can help please feel free to contact us at info@complete-physio.co.uk
Don’t let pain hold you back, book now!